A record of nootropics I have tried, with thoughts about which ones worked and did not work for me. These anecdotes should be considered only as anecdotes, and one’s efforts with nootropics a hobby to put only limited amounts of time into due to the inherent limits of drugs as a force-multiplier compared to other things like programming1; for an ironic counterpoint, I suggest the reader listen to a video of Jonathan Coulton’s“I Feel Fantastic” while reading.
Your mileage will vary. There are so many parameters and interactions in the brain that any of them could be the bottleneck or responsible pathway, and one could fall prey to the common U-shaped dose-response curve (eg. Yerkes-Dodson law; see also “Chemistry of the adaptive mind” & de Jongh et al 2008) which may imply that the smartest are those who benefit least23 but ultimately they all cash out in a very few subjective assessments like ‘energetic’ or ‘motivated’, with even apparently precise descriptions like ‘working memory’ or ‘verbal fluency’ not telling you much about what the nootropic actually did. It’s tempting to list the nootropics that worked for you and tell everyone to go use them, but that is merely generalizing from one example (and the more nootropics - or meditation styles, or self-help books, or “getting things done” systems - you try, the stronger the temptation is to evangelize). The best you can do is read all the testimonials and studies and use that to prioritize your list of nootropics to try. You don’t know in advance which ones will pay off and which will be wasted. You can’t know in advance. And wasted some must be; to coin a Umeshism: if all your experiments work, you’re just fooling yourself. (And the corollary - if someone else’s experiments always work, they’re not telling you everything.)
The above are all reasons to expect that even if I do excellent single-subject design self-experiments, there will still be the old problem of “internal validity” versus “external validity”: an experiment may be wrong or erroneous or unlucky in some way (lack of internal validity) or be right but not matter to anyone else (lack of external validity). For example, alcohol makes me sad & depressed; I could run the perfect blind randomized experiment for hundreds of trials and be extremely sure that alcohol makes me less happy, but would that prove that alcohol makes everyone sad or unhappy? Of course not, and as far as I know, for a lot of people alcohol has the opposite effect. So my hypothetical alcohol experiment might have tremendous internal validity (it does prove that I am sadder after inebriating), and zero external validity (someone who has never tried alcohol learns nothing about whether they will be depressed after imbibing). Keep this in mind if you are minded to take the experiments too seriously.
Somewhat ironically given the stereotypes, while I was in college I dabbled very little in nootropics, sticking to melatonin and tea. Since then I have come to find nootropics useful, and intellectually interesting: they shed light on issues in philosophy of biology & evolution, argue against naive psychological dualism and for materialism, offer cases in point on the history of technology & civilization or recent psychology theories about addiction & willpower, challenge our understanding of the validity of statistics and psychology - where they don’t offer nifty little problems in statistics and economics themselves, and are excellent fodder for the young Quantified Self movement45; modafinil itself demonstrates the underappreciated fact that sleep has no accepted evolutionary explanation. (The hard drugs also have more ramifications than one might expect: how can one understand the history of Southeast Asia and the Vietnamese War without reference to heroin, or more contemporaneously, how can one understand the lasting appeal of the Taliban in Afghanistan and the unpopularity & corruption of the central government without reference to the Taliban’s frequent anti-drug campaigns or the drug-funded warlords of the Northern Alliance?)
Nootropics have been around a long time, but they’ve never been so prominent, easily accessed, cheap, or available in such a variety. I think there is no single factor responsible but rather existing trends progressing to the point where it’s possible to obtain much more obscurer things than before.
(In particular, I don’t think it’s because there’s a sudden new surge of drugs. FDA drug approval has been decreasing over the past few decades, so this is unlikely a priori. More specifically, many of the major or hot drugs go back a long time. Bacopa goes back millennia, melatonin I don’t even know, piracetam was the ’60s, modafinil was ’70s or ’80s, ALCAR was ’80s AFAIK, Noopept & coluracetam were ’90s, and so on.)
What I see as being the relevant trends are a combination of these trends:
the rise of IP scofflaw countries which enable the manufacture of known drugs: India does not respect the modafinil patents, enabling the cheap generics we all use, and Chinese piracetam manufacturers don’t give a damn about the FDA’s chilling-effect moves in the US. If there were no Indian or Chinese manufacturers, where would we get our modafinil? Buy them from pharmacies at $10 a pill or worse? It might be worthwhile, but think of the chilling effect on new users.
along with the previous bit of globalization is an important factor: shipping is ridiculously cheap. The most expensive S&H in my modafinil price table is ~$15 (and most are international). To put this in perspective, I remember in the ‘90s you could easily pay $15 for domestic S&H when you ordered online - but it’s 2013, and the dollar has lost at least half its value, so in real terms, ordering from abroad may be like a quarter of what it used to cost, which makes a big difference to people dipping their toes in and contemplating a small order to try out this ’nootropics’ thing they’ve heard about.
as scientific papers become much more accessible online due to Open Access, digitization by publishers, and cheap hosting for pirates, the available knowledge about nootropics increases drastically. This reduces the perceived risk by users, and enables them to educate themselves and make much more sophisticated estimates of risk and side-effects and benefits. (Take my modafinil page: in 199729ya, how could an average person get their hands on any of the papers available up to that point? Or get detailed info like the FDA’s prescribing guide? Even assuming they had a computer & Internet?)
the larger size of the community enables economies of scale and increases the peak sophistication possible. In a small nootropics community, there is likely to be no one knowledgeable about statistics/experimentation/biochemistry/neuroscience/whatever-you-need-for-a-particular-discussion, and the available funds increase: consider /r/Nootropics’s testing program, which is doable only because it’s a large lucrative community to sell to so the sellers are willing to donate funds for independent lab tests/Certificates of Analysis (COAs) to be done. If there were 1,000 readers rather than 23,295, how could this ever happen short of one of those 1,000 readers being very altruistic?
Nootropics users tend to ‘stick’. If modafinil works well for you, you’re probably going to keep using it on and off. So simply as time passes, one would expect the userbase to grow. Similarly for press coverage and forum comments and blog posts: as time passes, the total mass increases and the more likely a random person is to learn of this stuff.
I do recommend a few things, like modafinil or melatonin, to many adults, albeit with misgivings about any attempt to generalize like that. (It’s also often a good idea to get powders, see the appendix.) Some of those people are helped; some have told me that they tried and the suggestion did little or nothing. I view nootropics as akin to a biological lottery; one good discovery pays for all.—I forged on in the hopes of further striking gold in my particular biology. Your mileage will vary. If you are interested, all you can do is to just try it. Most of my experiences were in my 20s as a right-handed 5’11 white male weighing 190–220lbs, fitness varying over time from not-so-fit to fairly fit. In rough order of personal effectiveness weighted by costs+side-effects, I rank them as follows:
Modafinil/armodafinil (less than weekly for overnight; skipping days for day use)
I mostly wound down my nootropics hobby around 201412ya as I switched to other topics (primarily AI). As of late 2024, I continue regular use of vitamin D/melatonin/caffeine+theanine/nicotine; after finally running out of my giant order of piracetam+choline, have dropped racetams because I’m not sure which one exactly I would want to use; and have been trying replacing sulbutiamine with a different (and inferior for me) thiamine derivative, benfotiamine, because sulbutiamine has become oddly difficult to buy, possibly due to the FDA.
(People aged <=18 shouldn’t be using any of this except harmless stuff - where one may have nutritional deficits - like fish oil & vitamin D; melatonin may be especially useful, thanks to the effects of screwed-up school schedules & electronics use on teenagers’ sleep. Changes in effects with age are real - amphetamines’ stimulant effects and modafinil’s histamine-like side-effects come to mind as examples.)
I’ve become increasingly skeptical of nootropics in general which aren’t either stimulants or addressing special cases (like vegetarians/creatine). This is partially due to modern genomics convincing me that intelligence and most other individual differences are driven by mutation load: just a ton of small bits of sand in the gears of everything, with intelligence as particularly acutely affected by problems upstream (eg. in mitochondria). For that sort of conception, it is extremely improbable to find any particular silver bullet. We also have yet to find any genetic mutations which boost intelligence by more than a trivial amount. On the other hand, personality/motivation seem somewhat more susceptible to modification because personality is in selection balance: unlike intelligence, where more is better, for every environment like the modern environment there is a certain amount of Extraversion which is optimal which is not being maximally Extraverted, say, there is a certain Conscientiousness level which is optimum to prevent slacking (but too much leads to behavioral inflexibility and sunk costs), and so on, and so there’s plenty of potential leeway for there to be something to modify motivation substantially, because evolution doesn’t ever want to modify motivation/personality too far from the population mean.
So, I don’t have any master list of particularly promising candidates. There’s nothing I think could be a silver bullet if only someone would run a proper study.
No effects, alone or mixed with choline+piracetam. This is pretty much as expected from reports about ALCAR (Examine.com), but I had still been hoping for energy boosts or something. (Bought from Smart Powders.)
Adderall is a mix of 4 amphetamine salts (FDA adverse events), and not much better than the others (but perhaps less addictive); as such, like caffeine or methamphetamine, it is not strictly a nootropic but a cognitive enhancer and can be tricky to use right (for how one should use stimulants, see “How To Take Ritalin Correctly”). I ordered 10x10mg Adderall IR off Silk Road (Wikipedia). On the 4th day after confirmation from seller, the package arrived. It was a harmless looking little padded mailer. Adderall as promised: 10 blue pills with markings, in a double ziplock baggy (reasonable, it’s not cocaine or anything). They matched pretty much exactly the descriptions of the generic I had found online. (Surprisingly, apparently both the brand name and the generic are manufactured by the same pharmacorp.)
I took the first pill at 12:48 pm. 1:18, still nothing really - head is a little foggy if anything. later noticed a steady sort of mental energy lasting for hours (got a good deal of reading and programming done) until my midnight walk, when I still felt alert, and had trouble sleeping. (Zeo reported a ZQ of 100, but a full 18 minutes awake, 2 or 3 times the usual amount.)
At this point, I began thinking about what I was doing. Black-market Adderall is fairly expensive; $4-10 a pill vs prescription prices which run more like $60 for 120 20mg pills. It would be a bad idea to become a fan without being quite sure that it is delivering bang for the buck. Now, why the piracetam mix as the placebo as opposed to my other available powder, creatine powder, which has much smaller mental effects? Because the question for me is not whether the Adderall works (I am quite sure that the amphetamines have effects!) but whether it works better for me than my cheap legal standbys (piracetam & caffeine)? (Does Adderall have marginal advantage for me?) Hence, I want to know whether Adderall is better than my piracetam mix. People frequently underestimate the power of placebo effects, so it’s worth testing. (Unfortunately, it seems that there is experimental evidence that people on Adderall know they are on Adderall and also believe they have improved performance, when they do not6. So the blind testing does not buy me as much as it could.)
But how to blind myself? I used my pill maker to make 9 OO pills of piracetam mix, and then 9 OO pills of piracetam mix+the Adderall, then I put them in a baggy. The idea is that I can blind myself as to what pill I am taking that day since at the end of the day, I can just look in the baggy and see whether a placebo or Adderall pill is missing: the big capsules are transparent so I can see whether there is a crushed-up blue Adderall in the end or not. If there are fewer Adderall than placebo, I took an Adderall, and vice-versa. Now, since I am checking at the end of each day, I also need to remove or add the opposite pill to maintain the ratio and make it easy to check the next day; more importantly I need to replace or remove a pill, because otherwise the odds will be skewed and I will know how they are skewed. (Imagine I started with 4 Adderalls and 4 placebos, and then 3 days in a row I draw placebos but I don’t add or remove any pills; the next day, because most of the placebos have been used up, there’s only a small chance I will get a placebo…)
This is only one of many ways to blind myself; for example, instead of using one bag, one could use two bags and instead blindly pick a bag to take a pill out of, balancing contents as before. (See also my Vitamin D and day modafinil trials.)
Began double-blind trial. Today I took one pill blindly at 1:53 PM. at the end of the day when I have written down my impressions and guess whether it was one of the Adderall pills, then I can look in the baggy and count and see whether it was. there are many other procedures one can take to blind oneself (have an accomplice mix up a sequence of pills and record what the sequence was; don’t count & see but blindly take a photograph of the pill each day, etc.) Around 3, I begin to wonder whether it was Adderall because I am arguing more than usual on IRC and my heart rate seems a bit high just sitting down. 6 PM: I’ve started to think it was a placebo. My heart rate is back to normal, I am having difficulty concentrating on long text, and my appetite has shown up for dinner (although I didn’t have lunch, I don’t think I had lunch yesterday and yesterday the hunger didn’t show up until past 7). Productivity wise, it has been a normal day. All in all, I’m not too sure, but I think I’d guess it was Adderall with 40% confidence (another way of saying ‘placebo with 60% confidence’). When I go to examine the baggie at 8:20 PM, I find out… it was an Adderall pill after all. Oh dear. One little strike against Adderall that I guessed wrong. It may be that the problem is that I am intrinsically a little worse today (normal variation? come down from Adderall?).
So, a change to the protocol. I will take a pill every other day - a day to washout and reacclimate to ‘baseline’, and then an experimental day. In subsequent entries, assume there was either an at least one intervening break or placebo day.
Took random pill at 2:02 PM. Went to lunch half an hour afterwards, talked until 4 - more outgoing than my usual self. I continued to be pretty energetic despite not taking my caffeine+piracetam pills, and though it’s now 12:30 AM and I listened to TAM YouTube videos all day while reading, I feel pretty energetic and am reviewing Mnemosyne cards. I am pretty confident the pill today was Adderall. Hard to believe placebo effect could do this much for this long or that normal variation would account for this. I’d say 90% confidence it was Adderall. I do some more Mnemosyne, typing practice, and reading in a Montaigne book, and finally get tired and go to bed around 1:30 AM or so. I check the baggie when I wake up the next morning, and sure enough, it had been an Adderall pill. That makes me 1 for 2.
Took pill 1:27 PM. At 2 my hunger gets the best of me (despite my usual tea drinking and caffeine+piracetam pills) and I eat a large lunch. This makes me suspicious it was placebo - on the previous days I had noted a considerable appetite-suppressant effect. 5:25 PM: I don’t feel unusually tired, but nothing special about my productivity. 8 PM; no longer so sure. Read and excerpted a fair bit of research I had been putting off since the morning. After putting away all the laundry at 10, still feeling active, I check. It was Adderall. I can’t claim this one either way. By 9 or 10 I had begun to wonder whether it was really Adderall, but I didn’t feel confident saying it was; my feeling could be fairly described as 50%.
Break; this day/night was for trying armodafinil, pill #1
Took pill around 6 PM; I had a very long drive to and from an airport ahead of me, ideal for Adderall. In case it was Adderall, I chewed up the pill - by making it absorb faster, more of the effect would be there when I needed it, during driving, and not lingering in my system past midnight. Was it? I didn’t notice any change in my pulse, I yawned several times on the way back, my conversation was not more voluminous than usual. I did stay up later than usual, but that’s fully explained by walking to get ice cream. All in all, my best guess was that the pill was placebo, and I feel fairly confident but not hugely confident that it was placebo. I’d give it ~70%. And checking the next morning… I was right! Finally.
Took pill 12:11 PM. I am not certain. While I do get some things accomplished (a fair amount of work on the Silk Road article and its submission to places), I also have some difficulty reading through a fiction book (Sum) and I seem kind of twitchy and constantly shifting windows. I am weakly inclined to think this is Adderall (say, 60%). It’s not my normal feeling. Next morning - it was Adderall.
Week-long break - armodafinil #2 experiment, volunteer work
Took pill #6 at 12:35 PM. Hard to be sure. I ultimately decided that it was Adderall because I didn’t have as much trouble as I normally would in focusing on reading and then finishing my novel (Surface Detail) despite my family watching a movie, though I didn’t notice any lack of appetite. Call this one 60-70% Adderall. I check the next evening and it was Adderall.
Took pill at 10:50 AM. At 12:30 I watch the new Captain America7, and come out as energetic as I went in and was not hungry for snacks at all during it; at this point, I’m pretty confident (70%) that it was Adderall. At 5 I check, and it was. Overall, pretty normal day, save for leading up to the third armodafinil trial.
Just 3 Adderall left; took random pill at 12:30. Hopefully I can get a lot of formatting done on hafu. I do manage to do a lot of work on it and my appetite seems minor up until 8 PM, although if not for those two observations; perhaps 60% that it was Adderall. I check the next morning, and it was not.
Skipping break day since it was placebo yesterday and I’d like to wind up the Adderall trials. Pill at 12:24 PM. I get very hungry around 3 PM, and it’s an unproductive day even considering how much stress and aggravation and the 3 hours a failed Debian unstable upgrade cost me. I feel quite sure (75%) it was placebo. It was.
Took pill at 11:27 AM. Moderately productive. Not entirely sure. 50% either way. (It’s placebo.)
Pill at 12:40 PM. I spend entirely too much time arguing matters related to a LW post and on IRC, but I manage to channel it into writing a new mini-essay on my past intellectual sins. This sort of thing seems like Adderall behavior, and I don’t get hungry until much later. All in all, I feel easily 75% sure it’s Adderall; and it was.
12:18 PM. (There are/were just 2 Adderall left now.) I manage to spend almost the entire afternoon single-mindedly concentrating on transcribing two parts of a 199630ya Toshio Okada interview (it was very long, and the formatting more challenging than expected), which is strong evidence for Adderall, although I did feel fairly hungry while doing it. I don’t go to bed until midnight and & sleep very poorly - despite taking triple my usual melatonin! Inasmuch as I’m already fairly sure that Adderall damages my sleep, this makes me even more confident (>80%). When I grumpily crawl out of bed and check: it’s Adderall. (One Adderall left.)
11:30 AM. By 2:30 PM, my hunger is quite strong and I don’t feel especially focused - it’s difficult to get through the tab-explosion of the morning, although one particularly stupid poster on the DNB ML makes me feel irritated like I might on Adderall. I initially figure the probability at perhaps 60% for Adderall, but when I wake up at 2 AM and am completely unable to get back to sleep, eventually racking up a Zeo score of 73 (compared to the usual 100s), there’s no doubt in my mind (95%) that the pill was Adderall. And it was the last Adderall pill indeed.
My predictions were substantially better than random chance8, so my default belief - that Adderall does affect me and (mostly) for the better - is borne out. I usually sleep very well and 3 separate incidents of horrible sleep in a few weeks seems rather unlikely (though I didn’t keep track of dates carefully enough to link the Zeo data with the Adderall data). Between the price and the sleep disturbances, I don’t think Adderall is personally worthwhile.
The amphetamine mix branded “Adderall” is terribly expensive to obtain even compared to modafinil, due to its tight regulation (a lower schedule than modafinil), popularity in college as a study drug, and reportedly moves by its manufacture to exploit its privileged position as a licensed amphetamine maker to extract more consumer surplus. I paid roughly $4 a pill but could have paid up to $10. Good stimulant hygiene involves recovery periods to avoid one’s body adapting to eliminate the stimulating effects, so even if Adderall was the answer to all my woes, I would not be using it more than 2 or 3 times a week. Assuming 50 uses a year (for specific projects, let’s say, and not ordinary aimless usage), that’s a cool $200 a year. My general belief was that Adderall would be too much of a stimulant for me, as I am amphetamine-naive and Adderall has a bad reputation for letting one waste time on unimportant things. We could say my prediction was 50% that Adderall would be useful and worth investigating further. The experiment was pretty simple: blind randomized pills, 10 placebo & 10 active. I took notes on how productive I was and the next day guessed whether it was placebo or Adderall before breaking the seal and finding out. I didn’t do any formal statistics for it, much less a power calculation, so let’s try to be conservative by penalizing the information quality heavily and assume it had 25%. So 200−0ln1.05⋅0.50⋅0.25=512! The experiment probably used up no more than an hour or two total.
Vaniver argues that since I start off not intending to continue Adderall, the analysis actually needs to be different:
In 3, you’re considering adding a new supplement, not stopping a supplement you already use. The “I don’t try Adderall” case has value $0, the “Adderall fails” case is worth −$40 (assuming you only bought 10 pills, and this number should be increased by your analysis time and a weighted cost for potential permanent side effects), and the “Adderall succeeds” case is worth $X-40-4099, where $X is the discounted lifetime value of the increased productivity due to Adderall, minus any discounted long-term side effect costs. If you estimate Adderall will work with p = 0.5, then you should try out Adderall if you estimate that 0.5⋅(X−4179)>0 → $X>4179$. (Adderall working or not isn’t binary, and so you might be more comfortable breaking down the various “how effective Adderall is” cases when eliciting X, by coming up with different levels it could work at, their values, and then using a weighted sum to get X. This can also give you a better target with your experiment- “this needs to show a benefit of at least Y from Adderall for it to be worth the cost, and I’ve designed it so it has a reasonable chance of showing that.”)
One thing to notice is that the default case matters a lot. This asymmetry is because you switch decisions in different possible worlds - when you would take Adderall but stop you’re in the world where Adderall doesn’t work, and when you wouldn’t take Adderall but do you’re in the world where Adderall does work (in the perfect information case, at least). One of the ways you can visualize this is that you don’t penalize tests for giving you true negative information, and you reward them for giving you true positive information. (This might be worth a post by itself, and is very Litany of Gendlin.)
Either way, this example demonstrates that anything you are doing expensively is worth testing extensively.
The adrafinil/Olmifon (bought simultaneously with the hydergine from Anti-Aging Systems, now Antiaging Central) was a disappointment. Almost as expensive as actual modafinil, with the risk of liver problems, but did nothing whatsoever that I noticed. It is supposed to be subtler than modafinil, but that’s a little ridiculous.
The advantage of adrafinil is that it is legal & over-the-counter in the USA, so one removes the small legal risk of ordering & possessing modafinil without a prescription, and the retailers may be more reliable because they are not operating in a niche of dubious legality. Based on comments from others, the liver problem may have been overblown, and modafinil vendors post-2012 seem to have become more unstable, so I may give adrafinil (from another source than Antiaging Central) a shot when my modafinil/armodafinil run out.
Based on this H+ article/advertisement, I gave a PEA supplement a try. Noticed nothing. Critical commentators pointed out that PEA was notoriously degraded by the digestive system and has essentially no effect on its own9, though Neurvana’s ‘pro’ supplement claimed to avoid that. I guess it doesn’t.
Discussions of PEA mention that it’s almost useless without a MAOI to pave the way; hence, when I decided to get deprenyl and noticed that deprenyl is a MAOI, I decided to also give PEA a second chance in conjunction with deprenyl. Unfortunately, in part due to my own shenanigans, Nubrain canceled the deprenyl order and so I have 20g of PEA sitting around. Well, it’ll keep until such time as I do get a MAOI.
Caffeine (Examine.com; FDA adverse events) is of course the most famous stimulant around and highly psychoactive, despite tolerating to an extreme extent.10 But consuming 200mg or more a day, I have discovered the downside: it is addictive and has a nasty withdrawal—headaches, decreased motivation, apathy, and general unhappiness. (It’s a little amusing to read academic descriptions of caffeine addiction11; if caffeine were a new drug, I wonder what Schedule it would be in and if people might be even more leery of it than modafinil.) Further, in some ways, aside from the ubiquitous placebo effect, caffeine combines a mix of weak performance benefits (Lorist & Snel 2008, Nehlig 2010) with some possible decrements, anecdotally and scientifically:
slows memory retrieval for unprimed memories (although it speeds retrieval for related/primed memories)
the usual U-curve applies to caffeine doses: eg. while a small dose of caffeine in energy drinks substantially improves reaction-time in the cued go/no-go task, higher doses improve reaction-time less and are much closer to baseline (their optimal tested dose is, for my weight of 93kg, ~100mg)
caffeine damages sleep (necessary for memory and alertness), even 6 hours before sleep
in rats, it inhibits memory formation in the hippocampusandinmice, although other mice saw mental benefits with improvement to “long-term memory when tested with object recognition”
Finally, it’s not clear that caffeine results in performance gains after long-term use; homeostasis/tolerance is a concern for all stimulants, but especially for caffeine. It is plausible that all caffeine consumption does for the long-term chronic user is restore performance to baseline. (Imagine someone waking up and drinking coffee, and their performance improves - well, so would the performance of a non-addict who is also slowly waking up!) See for example, James & Rogers 2005, Sigmon et al 2009, and Rogers et al 2010. A cross-section of thousands of participants in the Cambridge brain-training study found “caffeine intake showed negligible effect sizes for mean and component scores” (participants were not told to use caffeine, but the training was recreational & difficult, so one expects some difference).
This research is in contrast to the other substances I like, such as piracetam or fish oil. I knew about withdrawal of course, but it was not so bad when I was drinking only tea. And the side-effects like jitteriness are worse on caffeine without tea; I chalk this up to the lack of theanine. (My later experiences with theanine seems to confirm this.) These negative effects mean that caffeine doesn’t satisfy the strictest definition of ‘nootropic’ (having no negative effects), but is merely a ‘cognitive enhancer’ (with both benefits & costs). One might wonder why I use caffeine anyway if I am so concerned with mental ability, or don’t try expensive substitutes like paraxanthine?
My answer is that this is not a lot of research or very good research (not nearly as good as the research on nicotine, eg.), and assuming it’s true, I don’t value long-term memory that much because LTM is something that is easily assisted or replaced (personal archives, and spaced repetition). For me, my problems tend to be more about akrasia and energy and not getting things done, so even if a stimulant comes with a little cost to long-term memory, it’s still useful for me. I’m going continue to use the caffeine. It’s not so bad in conjunction with tea, is very cheap, and I’m already addicted, so why not? Caffeine is extremely cheap, addictive, has minimal effects on health (and may be beneficial, from the various epidemiological associations with tea/coffee/chocolate & longevity), and costs extra to remove from drinks popular regardless of their caffeine content (coffee and tea again). What would be the point of carefully investigating it? Suppose there was conclusive evidence on the topic, the value of this evidence to me would be roughly $0 or since ignorance is bliss, negative money - because unless the negative effects were drastic (which current studies rule out, although tea has other issues like fluoride or metal contents), I would not change anything about my life. Why? I enjoy my tea too much. My usual tea seller doesn’t even have decaffeinated oolong in general, much less various varieties I might want to drink, apparently because de-caffeinating is so expensive it’s not worthwhile. What am I supposed to do, give up my tea and caffeine just to save on the cost of caffeine? Buy de-caffeinating machines (which I couldn’t even find any prices for, googling)? This also holds true for people who drink coffee or caffeinated soda. (As opposed to a drug like modafinil which is expensive, and so the value of a definitive answer is substantial and would justify some more extensive calculating of cost-benefit.)
I ordered 400g of ‘anhydrous caffeine’ from Smart Powders. Apparently my oolong tea doesn’t contain very much caffeine, so adding a fraction of a gram wakes me up a bit. Surprisingly for something with ‘anhydrous’ in its name, it doesn’t seem to dissolve very well.
I ultimately mixed it in with the 3kg of piracetam and included it in that batch of pills. I mixed it very thoroughly, one ingredient at a time, so I’m not very worried about ‘hot spots’. But if you are, one clever way to get accurate caffeine measurements is to measure out a large quantity & dissolve it since it’s easier to measure water than powder, and dissolving guarantees even distribution. This can be important because caffeine is, like nicotine, an alkaloid poison which - “the dose makes the poison” - can kill in high doses, and concentrated powder makes it easy to take too much, as one inept Englishman discovered the hard way. (This dissolving trick is applicable to anything else that dissolves nicely.)
One of the more exotic nootropics popularly discussed back then was “Cerebrolysin”, an injected concotion of ‘peptides’ from pig brains.
I did not look into it in much detail: my needle phobia largely rules out any injectable, and it was also kinda expensive. But I was also skeptical of it. It was one of many dubious Eastern European/Russian ‘nootropics’, countries with well-earned reputations for low-quality & fraudulent research, exacerbated by the Putin kleptocracy eroding what norms there used to be, and nootropics are a particularly easy way to make a buck with snake oil. Further, while I’m no chemistry expert, I couldn’t understand how a slurry of random enzymatically-cut-up ‘peptides’ could possibly have any meaningful effect: if there was a specific peptide, perhaps, but just, a whole bunch of unknown peptides? Why would that have any particular consistent effect (as opposed to varying unpredictably from batch to batch and even injection to injection)? And if they are enzymatically degraded proteins, then why not just eat a steak? (Put it in a blender first to authentically recreate the lack of enjoyment.)
So I never looked into it much and I certainly never bought or injected any. In 2024, Greg Fitzgerald and Dan Elton did look into Cerebrolysin, and discussed a lot of historical information and also many alarming facts like an enormous level of fraud on many Cerebrolysin papers. All in all, I think there is enough evidence to firmly relegate Cerebrolysin to the trashcan.
Does little alone, but absolutely necessary in conjunction with piracetam. (Bought from Smart Powders.) When turning my 3kg of piracetam into pills, I decided to avoid the fishy-smelling choline and go with 500g of DMAE (Examine.com); it seemed to work well when I used it before with oxiracetam & piracetam, since I had no ‘piracetam headaches’, and be considerably less bulky.
In the future, I might try Alpha-GPC instead of the regular cholines; that supposedly has better bio-availability.
Chocolate or cocoa powder (Examine.com), contains the stimulants caffeine and the caffeine metabolite theobromine, so it’s not necessarily surprising if cocoa powder was a weak stimulant. It’s also a witch’s brew of chemicals such as polyphenols and flavonoids some of which have been fingered as helpful12, which all adds up to an unclear impact on health (once you control for eating a lot of sugar).
It’s not clear that there is much of an effect at all. This makes it hard to design a self-experiment - how big an effect on, say, dual n-back should I be expecting? Do I need an arduous long trial or an easy short one? This would principally determine the “value of information” too; chocolate seems like a net benefit even if it does not affect the mind, but it’s also fairly costly, especially if one likes (as I do) dark chocolate. Given the mixed research, I don’t think cocoa powder is worth investigating further as a nootropic.
Coconut oil was recommended by Pontus Granström on the Dual n-Back mailing list for boosting energy & mental clarity. It is fairly cheap (~$13 for 30 ounces) and tastes surprisingly good; it has a very bad reputation in some parts, but seems to be in the middle of a rehabilitation. Seth Robert’s Buttermind experiment found no mental benefits to coconut oil (and benefits to eating butter), but I wonder.
The first night I was eating some coconut oil, I did my n-backing past 11 PM; normally that damages my scores, but instead I got 66/66/75/88/77% (▁▁▂▇▃) on D4B and did not feel mentally exhausted by the end. The next day, I performed well on the Cambridge mental rotations test. An anecdote, of course, and it may be due to the vitamin D I simultaneously started. Or another day, I was slumped under apathy after a promising start to the day; a dose of fish & coconut oil, and 1 last vitamin D, and I was back to feeling chipper and optimist. Unfortunately I haven’t been testing out coconut oil & vitamin D separately, so who knows which is to thank. But still interesting.
After several weeks of regularly consuming coconut oil and using up the first jar of 15oz, I’m no longer particularly convinced it was doing anything. (I’ve found it’s good for frying eggs, though.) Several days after using up the second jar, I notice no real difference in mood or energy or DNB scores.
One of the most obscure -racetams around, coluracetam (Smarter Nootropics, Ceretropic, Isochroma) acts in a different way from piracetam - piracetam apparently attacks the breakdown of acetylcholine while coluracetam instead increases how much choline can be turned into useful acetylcholine. This apparently is an unique mechanism. A crazy Longecity user, ScienceGuy ponied up $16,000 (!) for a custom synthesis of 500g; he was experimenting with 10-80mg sublingual doses (the ranges in the original anti-depressive trials) and reported a laundry list of effects (as does Isochroma): primarily that it was anxiolytic and increased work stamina. Unfortunately for my stack, he claims it combines poorly with piracetam. He offered free 2g samples for regulars to test his claims. I asked & received some.
Experiment design is complicated by his lack of use of any kind of objective tests, but 3 metrics seem worthwhile:
dual n-back: testing his claims about concentration, increased energy & stamina, and increased alertness & lucidity.
daily Mnemosyne flashcard scores: testing his claim about short & medium-term memory, viz.
I have personally found that with respect to the NOOTROPIC effect(s) of all the RACETAMS, whilst I have experienced improvements in concentration and working capacity / productivity, I have never experienced a noticeable ongoing improvement in memory. COLURACETAM is the only RACETAM that I have taken wherein I noticed an improvement in MEMORY, both with regards to SHORT-TERM and MEDIUM-TERM MEMORY. To put matters into perspective, the memory improvement has been mild, yet still significant; whereas I have experienced no such improvement at all with the other RACETAMS.
daily mood/productivity log (1-5): for the anxiolytic and working claims.
(In all 3, higher = better, so a multivariate result is easily interpreted..)
He recommends a 10mg dose, but sublingually. He mentions “COLURACETAM’s taste is more akin to that of PRAMIRACETAM than OXIRACETAM, in that it tastes absolutely vile” (not a surprise), so it is impossible to double-blind a sublingual administration - even if I knew of an inactive equally-vile-tasting substitute, I’m not sure I would subject myself to it. To compensate for ingesting the coluracetam, it would make sense to double the dose to 20mg (turning the 2g into <100 doses). Whether the effects persist over multiple days is not clear; I’ll assume it does not until someone says it does, since this makes things much easier.
Creatine (Examine.com) monohydrate was another early essay of mine - cheap (because it’s so popular with the bodybuilder types), and with a very good safety record. I bought some from Bulk Powders and combined it with my then-current regimen (piracetam+choline). Creatine is a friendly powder with an inoffensive slightly chalky taste, and can be mixed into many drinks or even just taken directly. (It is not like many evil powders which are too foul or which ‘explode’ in the mouth.)
I’m not a bodybuilder, but my interest was sparked by several studies, some showing benefits and others not - usually in subpopulations like vegetarians or old people.
As I am not any of the latter, I didn’t really expect a mental benefit. As it happens, I observed nothing. What surprised me was something I had forgotten about: its physical benefits. My performance in Taekwondo classes suddenly improved - specifically, my endurance increased substantially. Before, classes had left me nearly prostrate at the end, but after, I was weary yet fairly alert and happy. (I have done Taekwondo since I was 7, and I have a pretty good sense of what is and is not normal performance for my body. This was not anything as simple as failing to notice increasing fitness or something.) This was driven home to me one day when in a flurry before class, I prepared my customary tea with piracetam, choline & creatine; by the middle of the class, I was feeling faint & tired, had to take a break, and suddenly, thunderstruck, realized that I had absentmindedly forgot to actually drink it! This made me a believer.
After I ran out of creatine, I noticed the increased difficulty, and resolved to buy it again at some point; many months later, there was a Smart Powders sale so bought it in my batch order, $12 for 1000g. As before, it made Taekwondo classes a bit easier. I paid closer attention this second time around and noticed that as one would expect, it only helped with muscular fatigue and did nothing for my aerobic issues. (I hate aerobic exercise, so it’s always been a weak point.) I eventually capped it as part of a sulbutiamine-DMAE-creatine-theanine mix. This ran out 2013-05-01. In March 201412ya, I spent $19 for 1kg of micronized creatine monohydrate to resume creatine use and also to use it as a placebo in a honey-sleep experiment testing Seth Roberts’s claim that a few grams of honey before bedtime would improve sleep quality: my usual flour placebo being unusable because the mechanism might be through simple sugars, which flour would digest into. (I did not do the experiment: it was going to be a fair amount of messy work capping the honey and creatine, and I didn’t believe Roberts’s claims for a second - my only reason to do it would be to prove the claim wrong but he’d just ignore me and no one else cares.) I didn’t try measuring out exact doses but just put a spoonful in my tea each morning (creatine is tasteless). The 1kg lasted from 25 March to 18 September or 178 days, so ~5.6g & $0.11 per day.
Cytisine is an obscure drug known, if at all, for use in anti-smoking treatment.
Cytisine is not known as a stimulant and I’m not addicted to nicotine, so why give it a try? Nicotine is one of the more effective stimulants available, and it’s odd how few nicotine analogues or nicotinic agonists there are available; nicotine has a few flaws like short half-life and increasing blood pressure, so I would be interested in a replacement. The nicotine metabolite cotinine, in the human studies available, looks intriguing and potentially better, but I have been unable to find a source for it. One of the few relevant drugs which I can obtain is cytisine, from Ceretropic, at 2x1.5mg doses. There are not many anecdotal reports on cytisine, but at least a few suggest somewhat comparable effects with nicotine, so I gave it a try.
My first dose on 2017-03-01, at the recommended 0.5ml/1.5mg was miserable, as I felt like I had the flu and had to nap for several hours before I felt well again, requiring 6h to return to normal; after waiting a month, I tried again, but after a week of daily dosing in May, I noticed no benefits; I tried increasing to 3x1.5mg but this immediately caused another afternoon crash/nap on 18 May. So I scrapped my cytisine. Oh well.
As far as anxiety goes, psychiatrist Emily Deans has an overview of why the Kiecolt-Glaser et al 201115ya study is nice; she also discusses why fish oil seems like a good idea from an evolutionary perspective. There was also a weaker earlier 200521ya study also using healthy young people, which showed reduced anger/anxiety/depression plus slightly faster reactions. The anti-stress/anxiolytic may be related to the possible cardiovascular benefits (Carter et al 2013).
I can test fish oil for mood, since the other claimed benefits like anti-schizophrenia are too hard to test. The medical student trial (Kiecolt-Glaser et al 201115ya) did not see changes until visit 3, after 3 weeks of supplementation. (Visit 1, 3 weeks, visit 2, supplementation started for 3 weeks, visit 3, supplementation continued 3 weeks, visit 4 etc.) There were no tests in between the test starting week 1 and starting week 3, so I can’t pin it down any further. This suggests randomizing in 2 or 3 week blocks. (For an explanation of blocking, see the footnote in the Zeo page.)
The placebos can be the usual pills filled with olive oil. The Nature’s Answer fish oil is lemon-flavored; it may be worth mixing in some lemon juice. In Kiecolt-Glaser et al 201115ya, ‘anxiety’ was measured via the Beck Anxiety scale; the placebo mean was 1.2 on a standard deviation of 0.075, and the experimental mean was 0.93 on a standard deviation of 0.076. (These are all log-transformed covariates or something; I don’t know what that means, but if I naively plug those numbers into Cohen’s d, I get a very large effect: 1.2−0.930.076=3.55.)
I noticed what may have been an effect on my dual n-back scores; the difference is not large (▃▆▃▃▂▂▂▂▄▅▂▄▂▃▅▃▄ vs ▃▄▂▂▃▅▂▂▄▁▄▃▅▂▃▂▄▂▁▇▃▂▂▄▄▃▃▂▃▂▂▂▃▄▄▃▆▄▄▂▃▄▃▁▂▂▂▃▂▄▂▁▁▂▄▁▃▂▄) and appears mostly in the averages - Toomim’s quick two-sample t-test gave p = 0.23, although an another analysis gives p = 0.138114. One issue with this before-after quasi-experiment is that one would expect my scores to slowly rise over time and hence a fish oil after would yield a score increase - the 3.2 point difference could be attributable to that, placebo effect, or random variation etc. But an accidentally noticed effect (d = 0.28) is a promising start. An experiment may be worth doing given that fish oil does cost a fair bit each year: randomized blocks permitting an fish-oil-then-placebo comparison would take care of the first issue, and then blinding (olive oil capsules versus fish oil capsules?) would take care of the placebo worry.
We have clear hypotheses here, so we can be a little optimistic: the fish oil will either improve mood or scores or it will do nothing; it will not worsen either. First, the large anxiety effect:
pwr.t.test(d=3.55,type="paired",power=0.75,alternative="greater",sig.level=0.05)# Paired t test power calculation## n = 2.269155## NOTE: n is number of *pairs*
Suspiciously easy. 2.25 pairs or 6 blocks? Let’s be pessimistic and use the smaller effect size estimate from my quasi-trial:
# pwr.t.test(d=0.28,type="paired",power=0.75,alternative="greater",sig.level=0.05)## Paired t test power calculation## n = 69.98612
70 pairs is 140 blocks; we can drop to 36 pairs or 72 blocks if we accept a power of 0.5/50% chance of reaching significance. (Or we could economize by hoping that the effect size is not 3.5 but maybe twice the pessimistic guess; a d = 0.5 at 50% power requires only 12 pairs of 24 blocks.) 70 pairs of blocks of 2 weeks, with 2 pills a day requires (70⋅2)⋅(2⋅7)⋅2=3920 pills. I don’t even have that many empty pills! I have <500; 500 would supply 250 days, which would yield 18 2-week blocks which could give 9 pairs. 9 pairs would give me a power of:
pwr.t.test(d=0.28,type="paired",alternative="greater",sig.level=0.05,n=9)# ... power = 0.1908962pwr.t.test(d=0.5,type="paired",alternative="greater",sig.level=0.05,n=9)# ... power = 0.3927739
For background on “value of information” calculations, see the Adderall calculation.
Cost of fish oil:
The price is not as good as multivitamins or melatonin. The studies showing effects generally use pretty high dosages, 1-4g daily. I took 4 capsules a day for roughly 4g of omega acids. The jar of 400 is 100 days’ worth, and costs ~$17, or around 17¢ a day. The general health benefits push me over the edge of favoring its indefinite use, but looking to economize. Usually, small amounts of packaged substances are more expensive than bulk unprocessed, so I looked at fish oil fluid products; and unsurprisingly, liquid is more cost-effective than pills (but like with the powders, straight fish oil isn’t very appetizing) in lieu of membership somewhere or some other price-break. I bought 4 bottles (16 fluid ounces each) for $53.31 total (thanks to coupons & sales), and each bottle lasts around a month and a half for perhaps half a year, or ~$100 for a year’s supply. (As it turned out, the 4 bottles lasted from 2010-12-04 to 2011-06-17, or 195 days.) My next batch lasted 2011-08–19-2012-02-20, and cost $58.27. Since I needed to buy empty 00 capsules (for my lithium experiment) and a book (Stanovich 2010, for SIAI work) from Amazon, I bought 4 more bottles of 16fl oz Nature’s Answer (lemon-lime) at $48.44, which I began using 2012-02-27. So call it ~$70 a year.
Most of the most solid fish oil results seem to meliorate the effects of age; in my 20s, I’m not sure they are worth the cost. But I would probably resume fish oil in my 30s or 40s when aging really becomes a concern. So the experiment at most will result in discontinuing for a decade. At $X a year, that’s a net present value of sum $ map (\n -> 70 / (1 + 0.05)^n) [1..10] = $540.5.
Cost of experimentation:
The fish oil can be considered a free sunk cost: I would take it in the absence of an experiment. The empty pill capsules could be used for something else, so we’ll put the 500 at $5. Filling 500 capsules with fish and olive oil will be messy and take an hour. Taking them regularly can be added to my habitual morning routine for vitamin D and the lithium experiment, so that is close to free but we’ll call it an hour over the 250 days. Recording mood/productivity is also free a sunk cost as it’s necessary for the other experiments; but recording dual n-back scores is more expensive: each round is ~2 minutes and one wants >=5, so each block will cost >10 minutes, so 18 tests will be >180 minutes or >3 hours. So >5 hours. Total: 5+(>5⋅7.25)=>41.
Priors:
The power calculation indicates a 20% chance of getting useful information. My quasi-experiment has <70% chance of being right, and I preserve a general skepticism about any experiment, even one as well done as the medical student one seems to be, and give that one a <80% chance of being right; so let’s call it 70% the effect exists, or 30% it doesn’t exist (which is the case in which I save money by dropping fish oil for 10 years).
Value of Information
Power times prior times benefit minus cost of experimentation: (0.20⋅0.30⋅540)−41=−9. So the VoI is negative: because my default is that fish oil works and I am taking it, weak information that it doesn’t work isn’t enough. If the power calculation were giving us 40% reliable information, then the chance of learning I should drop fish oil is improved enough to make the experiment worthwhile (going from 20% to 40% switches the value from −$9 to +$23.8).
The general cost of fish oil made me interested in possible substitutes. Seth Roberts uses exclusively flaxseed oil or flaxseed meal, and this seems to work well for him with subjective effects (eg. noticing his Chinese brands seemed to not work, possibly because they were unrefrigerated and slightly rancid). It’s been studied much less than fish oil, but omega acids are confusing enough in general (is there a right ratio? McCluskey’s roundup gives the impression claims about ratios may have been overstated) that I’m not convinced ALA is a much inferior replacement for fish oil’s mixes of EPA & DHA.
Flaxseed oil is, ounce for ounce, about as expensive as fish oil, and also must be refrigerated and goes bad within months anyway. Flax seeds on the other hand, do not go bad within months, and cost dollars per pound. Various resources I found online estimated that the ALA component of human-edible flaxseed to be around 20% So Amazon’s 6lbs for $14 is ~1.2lbs of ALA, compared to 16fl-oz of fish oil weighing ~1lb and costing ~$17, while also keeping better and being a calorically useful part of my diet. The flaxseeds can be ground in an ordinary food processor or coffee grinder. It’s not a hugely impressive cost-savings, but I think it’s worth trying when I run out of fish oil.
After trying out 2 6lb packs between 12 September & 2012-11-25, and 20 March & 2013-08-20, I have given up on flaxseed meal. They did not seem to go bad in the refrigerator or freezer, and tasted OK, but I had difficulty working them into my usual recipes: it doesn’t combine well with hot or cold oatmeal, and when I tried using flaxseed meal in soups I learned flaxseed is a thickener which can give soup the consistency of snot. It’s easier to use fish oil on a daily basis.
The chemical Huperzine-A (Examine.com) is extracted from a moss. It is an acetylcholinesterase inhibitor (instead of forcing out more acetylcholine like the -racetams, it prevents acetylcholine from breaking down). My experience report: One for the ‘null hypothesis’ files - Huperzine-A did nothing for me. Unlike piracetam or fish oil, after a full bottle (Source Naturals, 120 pills at 200μg each), I noticed no side-effects, no mental improvements of any kind, and no changes in DNB scores from straight Huperzine-A.
Possible confounding factors:
youth: I am considerably younger than the other poster who uses HA
I only tested a few days with choline+H-A (but I didn’t notice anything beyond the choline there).
counterfeiting? Source Naturals is supposed to be trustworthy, but rare herbal products are most susceptible to fake goods.
It’s really too bad. H-A is cheap, compact, doesn’t taste at all, and in general is much easier to take than fish oil (and much easier to swallow than piracetam or choline!). But if it doesn’t deliver, it doesn’t deliver.
As discussed in my iodine essay (FDA adverse events), iodine is a powerful health intervention as it eliminates cretinism and improves average IQ by a shocking magnitude. If this effect were possible for non-fetuses in general, it would be the best nootropic ever discovered, and so I looked at it very closely. Unfortunately, after going through ~20 experiments looking for ones which intervened with iodine post-birth and took measures of cognitive function, my meta-analysis concludes that: the effect is small and driven mostly by one outlier study. Once you are born, it’s too late. But the results could be wrong, and iodine might be cheap enough to take anyway, or take for non-IQ reasons. (This possibility was further weakened for me by an August 201313ya blood test of TSH which put me at 3.71 uIU/ml, comfortably within the reference range of 0.27-4.20.)
Starting from the studies in my meta-analysis, we can try to estimate an upper bound on how big any effect would be, if it actually existed. One of the most promising null results, Southon et al 199432ya, turns out to be not very informative: if we punch in the number of kids, we find that they needed a large effect size (d = 0.81) before they could see anything:
library(pwr)pwr.t.test(power=0.75, sig.level=0.05, n=22)# Two-sample t test power calculation## n = 22# d = 0.8130347
Fitzgerald 201214ya is better, and gives a number of useful details on her adult experiment:
Participants (n = 205) [young adults aged 18-30 years] were recruited between July 201016ya and January 201115ya, and were randomized to receive either a daily 150 μg (0.15mg) iodine supplement or daily placebo supplement for 32 weeks…After adjusting for baseline cognitive test score, examiner, age, sex, income, and ethnicity, iodine supplementation did not significantly predict 32 week cognitive test scores for Block Design (p = 0.385), Digit Span Backward (p = 0.474), Matrix Reasoning (p = 0.885), Symbol Search (p = 0.844), Visual Puzzles (p = 0.675), Coding (p = 0.858), and Letter-Number Sequencing (p = 0.408).
Full text isn’t available although some of the p-values suggest that there might be differences which didn’t reach significance, so to estimate an upper bound on what sort of effect-size we’re dealing with:
pwr.t.test(type="two.sample",power=0.75,alternative="greater",n=102)# Two-sample t test power calculation## n = 102# d = 0.325867
This is a much tighter upper bound than Southon et al 199432ya gave us, and also kind of discouraging: remember, the smaller the effect size, the more data you will need to see it, and data is always expensive. If I were to try to do any experiment, how many pairs would I need if we optimistically assume that d = 0.32?
pwr.t.test(type="paired",d=0.325867,power=0.75,alternative="greater")# Paired t test power calculation## n = 52.03677
We’d want 53 pairs, but Fitzgerald 2012’s experimental design called for 32 weeks of supplementation for a single pair of before-after tests - so that’d be 1664362ya weeks or ~54 months or ~4.5 years! We can try to adjust it downwards with shorter blocks allowing more frequent testing; but problematically, iodine is stored in the thyroid and can apparently linger elsewhere - many of the cited studies used intramuscular injections of iodized oil (as opposed to iodized salt or kelp supplements) because this ensured an adequate supply for months or years with no further compliance by the subjects. If the effects are that long-lasting, it may be worthless to try shorter blocks than ~32 weeks.
We’ve looked at estimating based on individual studies. But we aggregated them into a meta-analysis more powerful than any of them, and it gave us a final estimate of d=~0.1. What does that imply?
pwr.t.test(type="paired",d=0.1,power=0.75,alternative="greater")# Paired t test power calculation## n = 539.2906
540 pairs of tests or 1080 blocks… This game is not worth the candle!
For background on “value of information” calculations, see the Adderall calculation.
Cost:
This would be a very time-consuming experiment. Any attempt to combine this with other experiments by ANOVA would probably push the end-date out by months, and one would start to be seriously concerned that changes caused by aging or environmental factors would contaminate the results. A 5-year experiment with 7-month intervals will probably eat up 5+ hours to prepare <12,000 pills (active & placebo); each switch and test of mental functioning will probably eat up another hour for 32 hours. (And what test maintains validity with no practice effects over 5 years? Dual n-back would be unusable because of improvements to WM over that period.) Add in an hour for analysis & writeup, that suggests >38 hours of work, and 38⋅7.25=275.5. 12,000 pills is roughly $12.80 per thousand or $154; 120 potassium iodide pills is ~$9, so 365.25⧸120 × 9 × 5 = 137.
The time plus the gel capsules plus the potassium iodide is $567.
Benefit:
Some work has been done on estimating the value of IQ, both as net benefits to the possessor (including all zero-sum or negative-sum aspects) and as net positive externalities to the rest of society. The estimates are substantial: in the thousands of dollars per IQ point. But since increasing IQ post-childhood is almost impossible barring disease or similar deficits, and even increasing childhood IQs is very challenging, much of these estimates are merely correlations or regressions, and the experimental childhood estimates must be weakened considerably for any adult - since so much time and so many opportunities have been lost. A wild guess: $1,000 net present value per IQ point. The range for severely deficient children was 10-15 points, so any normal (somewhat deficient) adult gain must be much smaller and consistent with Fitzgerald 2012’s ceiling on possible effect sizes (small).
Let’s make another wild guess at 2 IQ points, for $2,000.
Expectation:
What is my prior expectation that iodine will do anything? A good way to break this question down is the following series of necessary steps:
how much do I believe I am iodine deficient?
(If I am not deficient, then supplementation ought to have no effect.) The previous material on modern trends suggests a prior >25%, and higher than that if I were female. However, I was raised on a low-salt diet because my father has high blood pressure, and while I like seafood, I doubt I eat it more often than weekly. I suspect I am somewhat iodine-deficient, although I don’t believe as confidently as I did that I had a vitamin D deficiency. Let’s call this one 75%.
If deficient, how likely would it help at my age?
(The effect may exist only at limited age ranges - like height, once you’re done growing, few interventions short of bone surgery will make one taller or shorter.) So this is one of the key assumptions: can we extend the benefits in deficient children to somewhat deficient adults?
Fitzgerald 201214ya and the general absence of successful experiments suggests not, as does the general historic failure of scores of IQ-related interventions in healthy young adults. Of the 10 studies listed in the original section dealing with iodine in children or adults, only 2 show any benefit; in lieu of a meta-analysis, a rule of thumb would be 20%, but both those studies used a package of dozens of nutrients - and not just iodine - so if the responsible substance were randomly picked, that suggests we ought to give it a chance of 20 of being iodine! I may be unduly optimistic if I give this as much as 10%.
If it would help at my age, how likely do I think my supplementation would hit the sweet spot and not under or overshoot?
(We already saw that too much iodine could poison both adults and children, and of course too little does not help much - iodine would seem to follow a U-curve like most supplements.) The listed doses at iherb.com often are ridiculously large: 10-50mg! These are doses that seems to actually be dangerous for long-term consumption, and I believe these are doses that are designed to completely suffocate the thyroid gland and prevent it from absorbing any more iodine - which is useful as a short-term radioactive fallout prophylactic, but quite useless from a supplementation standpoint. Fortunately, there are available doses at Fitzgerald 2012’s exact dose, which is roughly the daily RDA: 0.15mg. Even the contrarian materials seem to focus on a modest doubling or tripling of the existing RDA, so the range seems relatively narrow. I’m fairly confident I won’t overshoot if I go with 0.15-1mg, so let’s call this 90%.
Conclusion: 75% times 10% times 90% is 6.3%.
EV of taking iodine
Now, what is the expected value (EV) of simply taking iodine, without the additional work of the experiment? 4 cans of 0.15mg x 200 is $20 for 2.1 years’ worth or ~$10 a year or a NPV cost of $205 (10ln1.05) versus a 20% chance of $2,000 or $,400. So the expected value is greater than the NPV cost of taking it, so I should start taking iodine.
Value of Information
Finally, what is the value of information of conducting the experiment?
With an estimated power of 75%, and my own skeptical prior of 20% that there’s any effect worth caring about, and a potential benefit of $2,000, that’s 0.75⋅0.063⋅2000=95. We must weigh $95 against the estimated experimentation cost of $567. Since the information is worth less than the experiment costs, I should not do it.
But notice that most of the cost imbalance is coming from the estimate of the benefit of IQ - if it quadrupled to a defensible $8,000, that would be close to the experiment cost! So in a way, what this VoI calculation tells us is that what is most valuable right now is not that iodine might possibly increase IQ, but getting a better grip on how much any IQ intervention is worth.
So the overall picture is that I should:
start taking a moderate dose of iodine at some point
look into cheap tests for iodine deficiency
One self-test suggested online involves dripping iodine onto one’s skin and seeing how long it takes to be absorbed. This doesn’t seem terrible, but according to Derry and Abraham, it is unreliable.
Home urine test kits of unknown accuracy are available online (Google “iodine urine test kit”) but run $70-$100+ eg. Hakala Research.
try to think of cheaper experiments I could run for benefits from iodine
A poster or two on Longecity claimed that iodine supplementation had changed their eye color, suggesting a connection to the yellow-reddish element bromine - bromides being displaced by their chemical cousin, iodine. I was skeptical this was a real effect since I don’t know why visible amounts of either iodine or bromine would be in the eye, and the photographs produced were less than convincing. But it’s an easy thing to test, so why not?
For 2 weeks, upon awakening I took close-up photographs of my right eye. Then I ordered two jars of Life-Extension Sea-Iodine (60x1mg) (1mg being an apparently safe dose), and when it arrived on 2012-09-10, I stopped the photography and began taking 1 iodine pill every other day. I noticed no ill effects (or benefits) after a few weeks and upped the dose to 1 pill daily. After the first jar of 60 pills was used up, I switched to the second jar, and began photography as before for 2 weeks. The photographs were uploaded, cropped by hand in Gimp, and shrunk to more reasonable dimensions; both sets are available in a Zip file.
Upon examining the photographs, I noticed no difference in eye color, but it seems that my move had changed the ambient lighting in the morning and so there was a clear difference between the two sets of photographs! The ‘before’ photographs had brighter lighting than the ‘after’ photographs. Regardless, I decided to run a small survey on QuickSurveys/Toluna to confirm my diagnosis of no-change; the survey was 11 forced-choice pairs of photographs (before-after), with the instructions as follows:
Estimated time: <1 min.
Below is 11 pairs of close-up eye photographs,. In half the photos, the eye color of the iris may or may not have been artificially lightened; as a challenge, the photos are taken under varying light conditions!
In each pair, try to pick the photo with a lightened iris eye color if any. (Do not judge simply on overall lighting.)
(I reasoned that this description is not actually deceptive: taking pills is indeed “artificial”, as I would not ‘naturally’ consume so much iodine or seaweed extract, and I didn’t know for sure that my eyes hadn’t changed color so the correct description is indeed “may or may not have”.)
I posted a link to the survey on my Google+ account, and inserted the link at the top of all Gwern.net pages; 51 people completed all 11 binary choices (most of them coming from North America & Europe), which seems adequate since the 11 questions are all asking the same question, and 561 responses to one question is quite a few. A few different statistical tests seem applicable: a chi-squared test whether there’s a difference between all the answers, a two-sample test on the averages, and most meaningfully, summing up the responses as a single pair of numbers and doing a binomial test:
before <-c(27,31,18,26,22,29,20,13,18,31,27) # I split the 11 questions into how many picked,after <-c(24,20,33,25,29,22,31,38,33,20,24) # for it, before vs aftersummary(before); summary(after)# Min. 1st Qu. Median Mean 3rd Qu. Max.# 13.0 19.0 26.0 23.8 28.0 31.0# Min. 1st Qu. Median Mean 3rd Qu. Max.# 20.0 23.0 25.0 27.2 32.0 38.0chisq.test(before, after, simulate.p.value=TRUE)# Pearson`s Chi-squared test with simulated p-value## data: before and after# X-squared = 77, df = NA, p-value = 0.000135wilcox.test(before, after)# Wilcoxon rank sum test with continuity correction## data: before and after# W = 43, p-value = 0.2624# alternative hypothesis: true location shift is not equal to 0binom.test(c(sum(before), sum(after)))# Exact binomial test## data: c(sum(before), sum(after))# number of successes = 262, number of trials = 561, p-value = 0.1285# alternative hypothesis: true probability of success is not equal to 0.5# 95% confidence interval:# 0.4251 0.5093# sample estimates:# probability of success# 0.467
So the chi-squared believes there is a statistically-significant difference, the two-sample test disagrees, and the binomial also disagrees. Since I regarded it as a dubious theory, can’t see a difference, and the binomial seems like the most appropriate test, I conclude that several months of 1mg iodine did not change my eye color. (As a final test, when I posted the results on the Longecity forum where people were claiming the eye color change, I swapped the labels on the photos to see if anyone would claim something along the lines “when I look at the photos, I can see a difference!”. I thought someone might do that, which would be a damning demonstration of their biases & wishful thinking, but no one did.)
Kratom (Erowid, Reddit) is a tree leaf from Southeast Asia; it’s addictive to some degree (like caffeine and nicotine), and so it is regulated/banned in Thailand, Malaysia, Myanmar, and Bhutan among others - but not the USA. (One might think that kratom’s common use there indicates how very addictive it must be, except it literally grows on trees so it can’t be too hard to get.) Kratom is not particularly well-studied (and what has been studied is not necessarily relevant - I’m not addicted to any opiates!), and it suffers the usual herbal problem of being an endlessly variable food product and not a specific chemical with the fun risks of perhaps being poisonous, but in my reading it doesn’t seem to be particularly dangerous or have serious side-effects.
A LessWronger found that it worked well for him as far as motivation and getting things done went, as did another LessWronger who sells it online (terming it “a reasonable productivity enhancer”) as did one of his customers, a pickup artist oddly enough. The former was curious whether it would work for me too and sent me Speciosa Pro’s “Starter Pack: Test Drive” (a sampler of 14 packets of powder and a cute little wooden spoon). In SE Asia, kratom’s apparently chewed, but the powders are brewed as a tea.
I started with the 10g of ‘Vitality Enhanced Blend’, a sort of tan dust. Used 2 little-spoonfuls (dust tastes a fair bit like green/oolong tea dust) into the tea mug and then some boiling water. A minute of steeping and… bleh. Tastes sort of musty and sour. (I see why people recommended sweetening it with honey.) The effects? While I might’ve been more motivated - I hadn’t had caffeine that day and was a tad under the weather, a feeling which seemed to go away perhaps half an hour after starting - I can’t say I experienced any nausea or very noticeable effects. (At least the flavor is no longer quite so offensive.)
3 days later, I’m fairly miserable (slept poorly, had a hair-raising incident, and a big project was not received as well as I had hoped), so well before dinner (and after a nap) I brew up 2 wooden-spoons of ‘Malaysia Green’ (olive-color dust). I drank it down; tasted slightly better than the first. I was feeling better after the nap, and the kratom didn’t seem to change that.
The next day was somewhat similar, so at 2:40 I tried out 3 spoonfuls of ‘sm00th’ (?), a straight tan powder. Like the Malaysia Green, not so bad tasting. By the second cup, my stomach is growling a little. No particular motivation.
A week later: ‘Golden Sumatran’, 3 spoonfuls, a more yellowish powder. (I combined it with some tea dregs to hopefully cut the flavor a bit.) Had a paper to review that night. No (subjectively noticeable) effect on energy or productivity. I tried 4 spoonfuls at noon the next day; nothing except a little mental tension, for lack of a better word. I think that was just the harbinger of what my runny nose that day and the day before was, a head cold that laid me low during the evening.
4 spoons of ‘Thai Red Vein’ at 1:30 PM; cold hasn’t gone away but the acetaminophen was making it bearable.
4 spoons of ‘Enriched Thai’ (brown) at 8PM. Steeped 15 minutes, drank; no effect - I have to take a break to watch 3 Mobile Suit Gundam episodes before I even feel like working.
5 spoons of ‘Enriched Sumatran’ (tannish-brown) at 3:10 PM; especially sludgy this time, the Sumatran powder must be finer than the other.
4 spoons ‘Synergy’ (a “Premium Whole Leaf Blend”) at 11:20 AM; by 12:30 PM I feel quite tired and like I need to take a nap (previous night’s sleep was slightly above average, 96 ZQ).
5 spoons ‘Essential Indo’ (olive green) at 1:50 PM; no apparent effect except perhaps some energy for writing (but then a vague headache).
At dose #9, I’ve decided to give up on kratom. It is possible that it is helping me in some way that careful testing (eg. dual n-back over weeks) would reveal, but I don’t have a strong belief that kratom would help me (I seem to benefit more from stimulants, and I’m not clear on how an opiate-bearer like kratom could stimulate me). So I have no reason to do careful testing. Oh well.
Hericium erinaceus (Examine.com) was recommended strongly by several on the ImmInst.org forums for its long-term benefits to learning, apparently linked to Nerve growth factor. Highly speculative stuff, and it’s unclear whether the mushroom powder I bought was the right form to take (ImmInst.org discussions seem to universally assume one is taking an alcohol or hotwater extract). It tasted nice, though, and I mixed it into my sleeping pills (which contain melatonin & tryptophan). I’ll probably never know whether the $30 for 0.5lb was well-spent or not.
(I was more than a little nonplussed when the mushroom seller included a little pamphlet educating one about how papaya leaves can cure cancer, and how I’m shortening my life by decades by not eating many raw fruits & vegetables. There were some studies cited, but usually for points disconnected from any actual curing or longevity-inducing results.)
Lithium is a well-known mood stabilizer & suicide preventative; some research suggests lithium may be a cognitively-protective nutrient and on population levels chronic lithium consumption (through drinking water) predicts lower levels of mental illness, violence, & suicide. Main article: Lithium.
Lithium orotate is sold commercially in low-doses; I purchased 200 pills with 5mg of lithium each. (To put this dosage in comparison, the therapeutic psychiatric doses of lithium are around 500mg and roughly 100x larger.) The pills are small and tasteless, and not at all hard to take.
I experiment with a blind random trial of 5mg lithium orotate looking for effects on mood and various measures of productivity. There is no detectable effect, good or bad.
Some suggested that the lithium would turn me into a ‘zombie’, recalling the complaints of psychiatric patients. But at 5mg elemental lithium x 200 pills, I’d have to eat 20 to get up to a single clinical dose (a psychiatric dose might be 500mg of lithium carbonate, which translates to ~100mg elemental), so I’m not worried about overdosing. To test this, I took on day 1 & 2 no less than 4 pills/20mg as an attack dose; I didn’t notice any large change in emotional affect or energy levels. And it may’ve helped my motivation (though I am also trying out the tyrosine).
The effect? 3 or 4 weeks later, I’m not sure. When I began putting all of my nootropic powders into pill-form, I put half a lithium pill in each, and nevertheless ran out of lithium fairly quickly (3kg of piracetam makes for >4000 OO-size pills); those capsules were buried at the bottom of the bucket under lithium-less pills. So I suddenly went cold-turkey on lithium. Reflecting on the past 2 weeks, I seem to have been less optimistic and productive, with items now lingering on my To-Do list which I didn’t expect to. An effect? Possibly.
Most of the reported benefits of lithium are impossible for me to test: rates of suicide and Parkinson’s are right out, but so is crime and neurogenesis (the former is too rare & unusual, the latter too subtle & hard to measure), and likewise potential negatives. So we could measure:
mood, via daily self-report; should increase
The principal metric would be ‘mood’, however defined. Zeo’s web interface & data export includes a field for ‘Day Feel’, which is a rating 1-5 of general mood & quality of day. I can record a similar metric at the end of each day. 1-5 might be a little crude even with a year of data, so a more sophisticated measure might be in order. The first mood study is paywalled so I’m not sure what they used, but Shiotsuki 200818ya used State-Trait of Anxiety Inventory (STAI) and Profiles of Mood States Test (POMS). The full POMS sounds too long to use daily, but the Brief POMS might work. In the original 198739ya paper “A brief POMS measure of distress for cancer patients”, patients answering this questionnaire had a mean total mean of 10.43 (standard deviation 8.87). Is this the best way to measure mood? I’ve asked Seth Roberts; he suggested using a 0-100 scale, but personally, there’s no way I can assess my mood on 0-100. My mood is sufficiently stable (to me) that 0-5 is asking a bit much, even.
I ultimately decided to just go with the simple 0-5 scale, although it seems to have turned out to be more of a 2-4 scale! Apparently I’m not very good at introspection.
long-term memory (Mnemosyne 2.0’s statistics); could increase (neurogenesis), do nothing (null result), or decrease (metal poisoning)
working memory (dual n-back scores via Brain Workshop15); like long-term memory
sleep (Zeo); should increase (via mood improvement)
time procrastinating on computer (arbtt daemon every 10-40 seconds records open & active windows; these statistics can be parsed into categories like work or play. Total time on latter categories could be a useful metric. A second metric would be number of commits to the Gwern.net source repository.)
Lithium is somewhat persistent in the body, and its effects are not acute especially in low doses; this calls for long blocked trials.
The blood half-life is 12-36 hours; hence two or three days ought to be enough to build up and wash out. A week-long block is reasonable since that gives 5 days for effects to manifest, although month-long blocks would not be a bad choice either. (I prefer blocks which fit in round periods because it makes self-experiments easier to run if the blocks fit in normal time-cycles like day/week/month. The most useless self-experiment is the one abandoned halfway.)
With subtle effects, we need a lot of data, so we want at least half a year (6 blocks) or better yet, a year (12 blocks); this requires 180 actives and 180 placebos. This is easily covered by $11 for “Doctor’s Best Best Lithium Orotate (5mg), 200-Count” (more precisely, “Lithium 5mg (from 125mg of lithium orotate)”) and $14 for 1,000x1g empty capsules (purchased February 201214ya). For convenience I settled on 168 lithium & 168 placebos (7 pill-machine batches, 14 batches total); I can use them in 24 paired blocks of 7-days/1-week each (48 total blocks/48 weeks). The lithium expiration date is October 201412ya, so that is not a problem
The methodology would be essentially the same as the vitamin D in the morning experiment: put a multiple of 7 placebos in one container, the same number of actives in another identical container, hide & randomly pick one of them, use container for 7 days then the other for 7 days, look inside them for the label to determine which period was active and which was placebo, refill them, and start again.
For background on “value of information” calculations, see the Adderall calculation.
Low-dose lithium orotate is extremely cheap, ~$10 a year. There is some research literature on it improving mood and impulse control in regular people, but some of it is epidemiological (which implies considerable unreliability); my current belief is that there is probably some effect size, but at just 5mg, it may be too tiny to matter. I have ~40% belief that there will be a large effect size, but I’m doing a long experiment and I should be able to detect a large effect size with >75% chance. So, the formula is NPV of the difference between taking and not taking, times quality of information, times expectation: (10 − 0) ⧸ ln 1.05 × 0.75 × 0.40 = 61.4, which justifies a time investment of less than 9 hours. As it happens, it took less than an hour to make the pills & placebos, and taking them is a matter of seconds per week, so the analysis will be the time-consuming part. This one may actually turn a profit.
first block started and pill taken: 2012-05-11 - 19 May: 1
20 May - 27: 0
second pair
first block started and pill taken: 29 May - 4 June: 1
second block: 5 June - 11 June: 0
third pair
first block: 12 June - 18 June: 1
second block: 19 June - 25 June: 0
fourth pair
first block: 26 June - 2 July: 1
second block: 3 July - 8 July: 0
fifth pair
first block: 13 July - 20 July: 1
second block: 21 July - 27 July: 0
sixth pair
first block: 28 July - 3 August: 0
second block: 4 August - 10 August: 1
seventh pair
first block: 11 August - 17 August: 1
second block: 18 August - 24 August: 0
eighth pair
first block: 25 August - 31 August: 1
second block: 1 September - 4 September, stopped until 24 September, finished 25 September: 0
I interrupted the lithium self-experiment until March 201313ya in order to run the LSD microdosing self-experiment without a potential confound; ninth block pair:
arbtt generates cumulative time-usage for roughly a dozen overlapping tags/categories of activity of varying value. For the specific analysis, I plan to run factor analysis to extract one or two factors which seem to correlate with useful activity/work, and regress on those, instead of trying to regress on a dozen different time variables.
number of commits to the Gwern.net source repository
lithiumExperiment <-read.csv("https://gwern.net/doc/psychiatry/lithium/2012-lithium-experiment.csv")l1 <-lm(cbind(MP, Mnemosyne.grade, Gwern.net.patches, ZQ, MR3, MR2, MR4) ~ Lithium, data=lithiumExperiment)summary(l1)# Response MP :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 3.0613 0.0591 51.8 <2e-16# Lithium -0.0425 0.0841 -0.5 0.61## Residual standard error: 0.755 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.000796, Adjusted R-squared: -0.00233# F-statistic: 0.255 on 1 and 320 DF, p-value: 0.614### Response Mnemosyne.grade :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 3.158 0.120 26.41 <2e-16# Lithium -0.141 0.170 -0.83 0.41## Residual standard error: 1.53 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.00214, Adjusted R-squared: -0.000975# F-statistic: 0.687 on 1 and 320 DF, p-value: 0.408### Response Gwern.net.patches :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 3.8712 0.3271 11.83 <2e-16# Lithium 0.0345 0.4655 0.07 0.94## Residual standard error: 4.18 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 1.72e-05, Adjusted R-squared: -0.00311# F-statistic: 0.00549 on 1 and 320 DF, p-value: 0.941### Response ZQ :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 91.773 1.024 89.66 <2e-16# Lithium 0.523 1.457 0.36 0.72## Residual standard error: 13.1 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.000402, Adjusted R-squared: -0.00272# F-statistic: 0.129 on 1 and 320 DF, p-value: 0.72### Response MR3 :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) -0.0258 0.0691 -0.37 0.71# Lithium 0.0657 0.0983 0.67 0.50## Residual standard error: 0.882 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.00139, Adjusted R-squared: -0.00173# F-statistic: 0.447 on 1 and 320 DF, p-value: 0.504### Response MR2 :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 0.0187 0.0788 0.24 0.81# Lithium 0.0435 0.1121 0.39 0.70## Residual standard error: 1.01 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.00047, Adjusted R-squared: -0.00265# F-statistic: 0.15 on 1 and 320 DF, p-value: 0.698### Response MR4 :## Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 0.000209 0.052772 0.00 1.00# Lithium -0.073464 0.075099 -0.98 0.33## Residual standard error: 0.674 on 320 degrees of freedom# (220 observations deleted due to missingness)# Multiple R-squared: 0.00298, Adjusted R-squared: -0.000134# F-statistic: 0.957 on 1 and 320 DF, p-value: 0.329summary(manova(l1))# Df Pillai approx F num Df den Df Pr(>F)# Lithium 1 0.009477169 0.4291862 7 314 0.88373# Residuals 320
No variable reaches statistical-significance, the coefficient signs are inconsistent, and the MANOVA indicates no overall improvement by using the lithium variable.
There were no observable effects, either positive or beneficial, to the lithium orotate doses. This is consistent with my subjective experience. So I will not be using lithium orotate anymore.
An unusual intervention is infrared/near-infrared light of particular wavelengths (LLLT), theorized to assist mitochondrial respiration and yielding a variety of therapeutic benefits. Some have suggested it may have cognitive benefits. LLLT sounds strange but it’s simple, easy, cheap, and just plausible enough it might work. I tried out LLLT treatment on a sporadic basis 2013–201412ya, and statistically, usage correlated strongly & statistically-significantly with increases in my daily self-ratings, and not with any sleep disturbances. Excited by that result, I did a randomized self-experiment 2014–201511ya with the same procedure, only to find that the causal effect was weak or non-existent. I have stopped using LLLT as likely not worth the inconvenience.
Low level laser therapy (LLLT) is a curious treatment based on the application of a few minutes of weak light in specific near-infrared wavelengths (the name is a bit of a misnomer as LEDs seem to be employed more these days, due to the laser aspect being unnecessary and LEDs much cheaper). Unlike most kinds of light therapy, it doesn’t seem to have anything to do with circadian rhythms or zeitgebers. Proponents claim efficacy in treating physical injuries, back pain, and numerous other ailments, recently extending it to case studies of mental issues like brain fog. (It’s applied to injured parts; for the brain, it’s typically applied to points on the skull like F3 or F4.) And LLLT is, naturally, completely safe without any side effects or risk of injury.
To say that this all sounds dubious would be an understatement. (My first reaction was that LLLT and lostfalco’s other proposals were probably the stupidest thing I’d seen all month.)
The research literature, while copious, is messy and varied: methodologies and devices vary substantially, sample sizes are tiny, the study designs vary from paper to paper, metrics are sometimes comically limited (one study measured speed of finishing a RAPM IQ test but not scores), blinding is rare and unclear how successful, etc. Relevant papers include Chung et al 2012, Rojas & Gonzalez-Lima 2013, & Gonzalez-Lima & Barrett 2014. Another Longecity user ran a self-experiment, with some design advice from me, where he performed a few cognitive tests over several periods of LLLT usage (the blocks turned out to be ABBA), using his father and towels to try to blind himself as to condition. I analyzed his data, and his scores did seem to improve, but his scores improved so much in the last part of the self-experiment I found myself dubious as to what was going on - possibly a failure of randomness given too few blocks and an temporal exogenous factor in the last quarter which was responsible for the improvement.
While the mechanism is largely unknown, one commonly mechanism possibility is that light of the relevant wavelengths is preferentially absorbed by the protein cytochrome c oxidase, which is a key protein in mitochondrial metabolism and production of ATP, substantially increasing output, and this extra output presumably can be useful for cellular activities like healing or higher performance.
I was contacted by the Longecity user lostfalco, and read through some of his writings on the topic. I had never heard of LLLT before, but the mitochondria mechanism didn’t sound impossible (although I wondered whether it made sense at a quantity level16171819), and there was at least some research backing it; more importantly, lostfalco had discovered that devices for LLLT could be obtained as cheap as $15. (Clearly no one will be getting rich off LLLT or affiliate revenue any time soon.) Nor could I think of any way the LLLT could be easily harmful: there were no drugs involved, physical contact was unnecessary, power output was too low to directly damage through heating, and if it had no LLLT-style effect but some sort of circadian effect through hitting photoreceptors, using it in the morning wouldn’t seem to interfere with sleep.
Since LLLT was so cheap, seemed safe, was interesting, just trying it would involve minimal effort, and it would be a favor to lostfalco, I decided to try it. I purchased off eBay a $13 “48 LED illuminator light IR Infrared Night Vision+Power Supply For CCTV. Auto Power-On Sensor, only turn-on when the surrounding is dark. IR LED wavelength: 850nm. Powered by DC 12V 500mA adaptor.” It arrived in 4 days, on 2013-09-07. It fits handily in my palm. My cellphone camera verified it worked and emitted infrared - important because there’s no visible light at all (except in complete darkness I can make out a faint red light), no noise, no apparent heat (it took about 30 minutes before the lens or body warmed up noticeably when I left it on a table). This was good since I worried that there would be heat or noise which made blinding impossible; all I had to do was figure out how to randomly turn the power on and I could run blinded self-experiments with it.
My first time was relatively short: 10 minutes around the F3/F4 points, with another 5 minutes to the forehead. Awkward holding it up against one’s head, and I see why people talk of “LED helmets”, it’s boring waiting. No initial impressions except maybe feeling a bit mentally cloudy, but that goes away within 20 minutes of finishing when I took a nap outside in the sunlight. Lostfalco says “Expectations: You will be tired after the first time for 2 to 24 hours. It’s perfectly normal.”, but I’m not sure - my dog woke me up very early and disturbed my sleep, so maybe that’s why I felt suddenly tired. On the second day, I escalated to 30 minutes on the forehead, and tried an hour on my finger joints. No particular observations except less tiredness than before and perhaps less joint ache. Third day: skipped forehead stimulation, exclusively knee & ankle. Fourth day: forehead at various spots for 30 minutes; tiredness 5/6/7/8th day (11/12/13/4): skipped. Ninth: forehead, 20 minutes. No noticeable effects.
At this point I began to get bored with it and the lack of apparent effects, so I began a pilot trial: I’d use the LED set for 10 minutes every few days before 2PM, record, and in a few months look for a correlation with my daily self-ratings of mood/productivity (for 2.5 years I’ve asked myself at the end of each day whether I did more, the usual, or less work done that day than average, so 2=below-average, 3=average, 4=above-average; it’s ad hoc, but in some factor analyses I’ve been playing with, it seems to load on a lot of other variables I’ve measured, so I think it’s meaningful).
On 2014-03-15, I disabled light sensor: the complete absence of subjective effects since the first sessions made me wonder if the LED device was even turning on - a little bit of ambient light seems to disable it thanks to the light sensor. So I stuffed the sensor full of putty, verified it was now always-on with the cellphone camera, and began again; this time it seemed to warm up much faster, making me wonder if all the previous sessions’ sense of warmth was simply heat from my hand holding the LEDs
In late July 201412ya, I was cleaning up my rooms and was tired of LLLT, so I decided to chuck the LED device. But before I did that, I might as well analyze the data.
That left me with 329 days of data. The results are that (correcting for the magnesium citrate self-experiment I was running during the time period which did not turn out too great) days on which I happened to use my LED device for LLLT were much better than regular days. Below is a graph showing the entire MP dataseries with LOESS-smoothed lines showing LLLT vs non-LLLT days:
Daily productivity self-rating (higher=better) over time, split by LLLT usage that day (2013–201412ya)
The correlation of LLLT usage with higher MP self-rating is fairly large (r = 0.19 / d = 0.455) and statistically-significant (p = 0.0006).
I have no particularly compelling story for why this might be a correlation and not causation. It could be placebo, but I wasn’t expecting that. It could be selection effect (days on which I bothered to use the annoying LED set are better days) but then I’d expect the off-days to be below-average and compared to the 2 years of trendline before, there doesn’t seem like much of a fall.
The R code:
lllt <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2014-08-03-lllt-correlation.csv")l <-lm(MP ~ LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date),data=lllt); summary(l)# ...Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 4.037702597 0.616058589 6.55409 5.0282e-10# LLLTTRUE 0.330923350 0.095939634 3.44929 0.00069087# as.logical(Magnesium.citrate)TRUE 0.963379487 0.842463568 1.14353 0.25424378# as.integer(Date) -0.001269089 0.000880949 -1.44059 0.15132856# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.001765953 0.001213804 -1.45489 0.147332120.330923350/sd(lllt$MP, na.rm=TRUE)# [1] 0.455278787cor.test(lllt$MP, as.integer(lllt$LLLT))## Pearson`s product-moment correlation## data: lllt$MP and as.integer(lllt$LLLT)# t = 3.4043, df = 327, p-value = 0.0007458# alternative hypothesis: true correlation is not equal to 0# 95% confidence interval:# 0.0784517682 0.2873891665# sample estimates:# cor# 0.185010342## check whether there's odd about non-LLLT days by expanding to include baselinellltImputed <- llltllltImputed[is.na(llltImputed)] <-0llltImputed[llltImputed$MP ==0,]$MP <-3# clean up an outlier using mediansummary(lm(MP ~ LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date),data=llltImputed))# ...Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 2.959172295 0.049016571 60.37085 < 2.22e-16# LLLT 0.336886970 0.083731179 4.02344 6.2212e-05# as.logical(Magnesium.citrate)TRUE 2.155586397 0.619675529 3.47857 0.00052845# as.integer(Date) 0.000181441 0.000103582 1.75166 0.08017565# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.003373682 0.000904342 -3.73054 0.00020314power.t.test(power=0.8,delta=(0.336886970/sd(lllt$MP, na.rm=TRUE)),type="paired",alternative="one.sided")## Paired t test power calculation## n = 30.1804294# delta = 0.463483435# sd = 1# sig.level = 0.05# power = 0.8# alternative = one.sided## NOTE: n is number of *pairs*, sd is std.dev. of *differences* within pairslibrary(ggplot2)llltImputed$Date <-as.Date(llltImputed$Date)ggplot(data = llltImputed, aes(x=Date, y=MP, col=as.logical(llltImputed$LLLT))) +geom_point(size=I(3)) +stat_smooth() +scale_colour_manual(values=c("gray49", "green"),name ="LLLT")
So, I have started a randomized experiment; should take 2 months, given the size of the correlation. If that turns out to be successful too, I’ll have to look into methods of blinding - for example, some sort of electronic doohickey which turns on randomly half the time and which records whether it’s on somewhere one can’t see. (Then for the experiment, one hooks up the LED, turns the doohickey ‘on’, and applies directly to forehead, checking the next morning to see whether it was really on or off).
One reader notes that for her, the first weeks of LLLT usage seemed to be accompanied by sleeping longer than usual. Did I experience anything similar? There doesn’t appear to be any particular effect on total sleep or other sleep variables:
Factor-analyzing several other personal datasets into 8 factors while omitting the previous MP variable, I find LLLT correlates with personal-productivity-related factors, but less convincingly than MP, suggesting the previous result is not quite as good as it seems.
My worry about the MP variable is that, plausible or not, it does seem relatively weak against manipulation; other variables I could look at, like arbtt window-tracking of how I spend my computer time, # or size of edits to my files, or spaced repetition performance, would be harder to manipulate. If it’s all due to MP, then if I remove the MP and LLLT variables, and summarize all the other variables with factor analysis into 2 or 3 variables, then I should see no increases in them when I put LLLT back in and look for a correlation between the factors & LLLT with a multivariate regression.
Preparation of data:
lllt <-read.csv("~/wiki/doc/nootropic/quantified-self/2014-08-03-lllt-correlation.csv",colClasses=c("Date",rep("integer", 4), "logical"))lllt <-data.frame(Date=lllt$Date, LLLT=lllt$LLLT)mp <-read.csv("~/selfexperiment/mp.csv", colClasses=c("Date", "integer"))creativity <-read.csv("~/selfexperiment/dailytodo-marchjunecreativity.csv",colClasses=c("Date", "integer"))mnemosyne <-read.csv("~/selfexperiment/mnemosyne.csv", header=FALSE,col.names =c("Timestamp", "Easiness", "Grade"),colClasses=c("integer", "numeric", "integer"))mnemosyne$Timestamp <-as.POSIXct(mnemosyne$Timestamp, origin ="1970-01-01", tz ="EST")mnemosyne$Date <-as.Date(mnemosyne$Timestamp)mnemosyne <-aggregate(Grade ~ Date, mnemosyne, mean)mnemosyne$Average.Spaced.repetition.score <- mnemosyne$Graderm(mnemosyne$Grade)dnb <-read.csv("~/doc/brainworkshop/data/stats.txt", header=FALSE)dnb$V1 <-as.POSIXct(dnb$V1, format="%F %R:%S")dnb <- dnb[!is.na(dnb$V1),]dnb <-with(dnb, data.frame(Timestamp=V1, Nback.type=V2, Percentage=V3))dnb$Date <-as.Date(dnb$Timestamp)dnbDaily <-aggregate(Percentage ~ Date + Nback.type, dnb, mean)arbtt1 <-read.csv("~/selfexperiment/2012-2013-arbtt.txt")arbtt2 <-read.csv("~/selfexperiment/2013-2014-arbtt.txt")arbtt <-rbind(arbtt1, arbtt2)rm(arbtt$Percentage)interval <-function(x) { if (!is.na(x)) { if (grepl(" s",x)) as.integer(sub(" s","",x))else { y <-unlist(strsplit(x, ":"));as.integer(y[[1]])*3600+as.integer(y[[2]])*60+as.integer(y[[3]]); } }elseNA }arbtt$Time <-sapply(as.character(arbtt$Time), interval)library(reshape)arbtt <-reshape(arbtt, v.names="Time", timevar="Tag", idvar="Day", direction="wide")arbtt$Date <-as.Date(arbtt$Day)rm(arbtt$Day)arbtt[is.na(arbtt)] <-0patches <-read.csv("~/selfexperiment/patchlog-gwern.net.txt", colClasses=c("integer", "Date"))patches$Gwern.net.patches.log <-log1p(patches$Gwern.net.patches)# modified lines per day is much harder: state machine to sum lines until it hits the next datepatchCount <-scan(file="~/selfexperiment/patchlog-linecount-gwern.net.txt", character(), sep ="\n")patchLines <-new.env()for (i in1:length(patchCount)) {if (grepl("\t", patchCount[i])) { patchLines[[date]] <- patchLines[[date]] +sum(sapply(strsplit(patchCount[i], "\t"), as.integer)) }else { date <- patchCount[i] patchLines[[date]] <-0 } }patchLines <-as.list(patchLines)patchLines <-data.frame(Date =rep(names(patchLines), lapply(patchLines, length)),Gwern.net.linecount=unlist(patchLines))rm(row.names(patchLines))patchLines$Date <-as.Date(patchLines$Date)patchLines$Gwern.net.linecount.log <-log1p(patchLines$Gwern.net.linecount)firstDay <- patches$Date[1]; lastDay <- patches$Date[nrow(patches)]patches <-merge(merge(patchLines, patches, all=TRUE), data.frame(Date=seq(firstDay, lastDay, by="day")), all=TRUE)# if entries are missing, they == 0patches[is.na(patches)] <-0# combine all the data:llltData <-merge(merge(merge(merge(merge(lllt, mp, all=TRUE), creativity, all=TRUE), dnbDaily, all=TRUE), arbtt, all=TRUE), patches, all=TRUE)write.csv(llltData, file="2014-08-08-lllt-correlation-factoranalysis.csv", row.names=FALSE)
Factor analysis. The strategy: read in the data, drop unnecessary data, impute missing variables (data is too heterogeneous and collected starting at varying intervals to be clean), estimate how many factors would fit best, factor analyze, pick the ones which look like they match best my ideas of what ‘productive’ is, extract per-day estimates, and finally regress LLLT usage on the selected factors to look for increases.
lllt <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2014-08-08-lllt-correlation-factoranalysis.csv")## the log transforms are more useful:rm(lllt$Date, lllt$Nback.type, lllt$Gwern.net.linecount, lllt$Gwern.net.patches)## https://stats.stackexchange.com/questions/28576/filling-nas-in-a-dataset-with-column-medians-in-rimputeColumnAsMedian <-function(x){ x[is.na(x)] <-median(x, na.rm=TRUE) #convert the item with NA to median value from the column x #display the column}llltI <-data.frame(apply(lllt, 2, imputeColumnAsMedian))library(psych)nfactors(llltI[-c(1,2)])# VSS complexity 1 achieves a maximum of 0.56 with 16 factors# VSS complexity 2 achieves a maximum of 0.66 with 16 factors# The Velicer MAP achieves a minimum of 0.01 with 1 factors# Empirical BIC achieves a minimum of -280.23 with 8 factors# Sample Size adjusted BIC achieves a minimum of -135.77 with 9 factorsfa.parallel(llltI[-c(1,2)], n.iter=2000)# Parallel analysis suggests that the number of factors = 7 and the number of components = 7## split the difference between sample-size adjusted BIC and parallel analysis with 8:factorization <-fa(llltI[-c(1,2)], nfactors=8); factorization# Standardized loadings (pattern matrix) based upon correlation matrix# MR6 MR1 MR2 MR4 MR3 MR5 MR7 MR8 h2 u2 com# Creativity.self.rating 0.22 0.06 -0.04 0.08 -0.04 0.02 -0.05 -0.14 0.0658 0.934 2.5# Percentage -0.05 -0.02 0.01 0.01 0.00 -0.42 0.02 0.02 0.1684 0.832 1.0# Time.X -0.04 0.11 0.04 0.88 -0.02 0.01 0.01 0.02 0.8282 0.172 1.0# Time.PDF 0.02 0.99 -0.02 0.04 0.02 0.00 -0.01 -0.01 0.9950 0.005 1.0# Time.Stats -0.10 0.21 0.12 0.16 -0.04 0.04 0.12 0.25 0.2310 0.769 4.3# Time.IRC 0.01 -0.02 0.99 0.02 0.02 0.01 0.00 -0.01 0.9950 0.005 1.0# Time.Writing 0.01 -0.02 0.01 0.04 -0.01 -0.03 0.68 0.04 0.4720 0.528 1.0# Time.Rec 0.20 -0.12 -0.06 0.42 0.62 -0.02 -0.07 -0.01 0.8501 0.150 2.2# Time.Music -0.05 0.05 0.02 0.02 -0.04 0.22 0.02 0.13 0.0909 0.909 2.0# Time.SRS -0.07 0.09 0.08 0.00 0.00 0.08 0.06 0.16 0.0702 0.930 3.6# Time.Sysadmin 0.05 -0.09 -0.04 0.15 0.07 0.01 0.14 0.42 0.2542 0.746 1.7# Time.Bitcoin 0.45 0.02 0.25 -0.07 -0.03 -0.09 -0.04 0.11 0.3581 0.642 1.9# Time.Backups 0.22 0.10 -0.08 -0.19 0.12 0.13 0.02 0.27 0.1809 0.819 4.3# Time.Blackmarkets 0.62 -0.01 0.06 -0.02 -0.09 -0.01 -0.04 0.15 0.4442 0.556 1.2# Time.Programming 0.06 -0.01 -0.01 -0.04 0.07 0.08 0.41 -0.07 0.1790 0.821 1.3# Time.DNB -0.01 -0.01 0.02 0.01 -0.01 0.76 -0.01 0.00 0.5800 0.420 1.0# Time.Typing -0.04 0.05 0.02 0.01 -0.02 -0.01 0.00 -0.01 0.0054 0.995 2.9# Time.Umineko -0.10 0.08 0.06 -0.15 0.77 -0.01 0.03 0.02 0.5082 0.492 1.2# Gwern.net.linecount.log 0.65 0.03 0.00 -0.03 0.04 0.00 0.10 -0.13 0.4223 0.578 1.1# Gwern.net.patches.log 0.11 0.02 -0.01 0.02 0.00 0.06 0.29 -0.06 0.1001 0.900 1.5## MR6 MR1 MR2 MR4 MR3 MR5 MR7 MR8# SS loadings 1.24 1.12 1.13 1.13 1.05 0.86 0.80 0.48# Proportion Var 0.06 0.06 0.06 0.06 0.05 0.04 0.04 0.02# Cumulative Var 0.06 0.12 0.17 0.23 0.28 0.33 0.37 0.39# Proportion Explained 0.16 0.14 0.14 0.14 0.13 0.11 0.10 0.06# Cumulative Proportion 0.16 0.30 0.45 0.59 0.73 0.84 0.94 1.00## With factor correlations of# MR6 MR1 MR2 MR4 MR3 MR5 MR7 MR8# MR6 1.00 -0.13 0.26 0.15 0.22 -0.09 0.03 0.16# MR1 -0.13 1.00 -0.12 0.25 -0.05 0.06 0.12 0.11# MR2 0.26 -0.12 1.00 0.04 -0.04 0.10 0.20 0.19# MR4 0.15 0.25 0.04 1.00 0.32 0.01 -0.05 0.10# MR3 0.22 -0.05 -0.04 0.32 1.00 -0.04 -0.07 0.00# MR5 -0.09 0.06 0.10 0.01 -0.04 1.00 0.11 0.11# MR7 0.03 0.12 0.20 -0.05 -0.07 0.11 1.00 0.20# MR8 0.16 0.11 0.19 0.10 0.00 0.11 0.20 1.00## Mean item complexity = 1.9# Test of the hypothesis that 8 factors are sufficient.## The degrees of freedom for the null model are 190# and the objective function was 2.46 with Chi Square of 5344.68# The degrees of freedom for the model are 58 and the objective function was 0.07## The root mean square of the residuals (RMSR) is 0.02# The df corrected root mean square of the residuals is 0.03## The harmonic number of observations is 2178 with the empirical chi square 190.08 with prob < 5.9e-16# The total number of observations was 2178 with MLE Chi Square = 149.65 with prob < 4.9e-10## Tucker Lewis Index of factoring reliability = 0.942# RMSEA index = 0.027 and the 90 % confidence intervals are 0.022 0.032# BIC = -296.15# Fit based upon off diagonal values = 0.98# Measures of factor score adequacy# MR6 MR1 MR2 MR4 MR3 MR5 MR7 MR8# Correlation of scores with factors 0.84 1.00 1.00 0.93 0.89 0.80 0.76 0.64# Multiple R square of scores with factors 0.70 0.99 0.99 0.86 0.79 0.63 0.58 0.41# Minimum correlation of possible factor scores 0.40 0.99 0.99 0.71 0.58 0.27 0.16 -0.19
The important factors seem to be: #1/MR6 (Creativity.self.rating, Time.Bitcoin, Time.Backups, Time.Blackmarkets, Gwern.net.linecount.log), #2/MR1 (Time.PDF, Time.Stats), #7/MR7 (Time.Writing, Time.Sysadmin, Time.Programming, Gwern.net.patches.log), and #8/MR8 (Time.States, Time.SRS, Time.Sysadmin, Time.Backups, Time.Blackmarkets). The rest seem to be time-wasting or reflect dual n-back/DNB usage (which is not relevant in the LLLT time period).
So we want to extract and look at factors #1/2/7/8 (MR6/1/7/8):
All of the coefficients are positive, as one would hope, and one specific factor (MR7) squeaks in at d = 0.34 (p = 0.05). The graph is much less impressive than the graph for just MP, suggesting that the correlation may be spread out over a lot of factors, the current dataset isn’t doing a good job of capturing the effect compared to the MP self-rating, or it really was a placebo effect:
Daily MR7 activity (writing/programming) factor correlated with LLLT usage (2013–201412ya)
A randomized non-blind self-experiment of LLLT 2014–201511ya yields a causal effect which is several times smaller than a correlative analysis and non-statistically-significant/very weak Bayesian evidence for a positive effect. This suggests that the earlier result had been driven primarily by reverse causation, and that my LLLT usage has little or no benefits.
Following up on the promising but unrandomized pilot, I began randomizing my LLLT usage since I worried that more productive days were causing use rather than vice-versa. I began on 2014-08-02, and the last day was 2015-03-03 (n = 167); this was twice the sample size I thought I needed, and I stopped, as before, as part of cleaning up (I wanted to know whether to get rid of it or not). The procedure was simple: by noon, I flipped a bit and either did or did not use my LED device; if I was distracted or didn’t get around to randomization by noon, I skipped the day. This was an unblinded experiment because finding a randomized on/off switch is tricky/expensive and it was easier to just start the experiment already. The question is simple too: controlling for the simultaneous blind magnesium experiment & my rare nicotine use (I did not use modafinil during this period or anything else I expect to have major influence), is the pilot correlation of d = 0.455 on my daily self-ratings borne out by the experiment?
Daily productivity self-rating (higher=better) over time, split by LLLT usage that day (2014–201511ya)
llltRandom <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2015-lllt-random.csv",colClasses=c("Date", "logical", "integer", "logical", "logical"))# impute magnesium data: that randomized experiment started a month laterllltRandom[is.na(llltRandom$Magnesium.random),]$Magnesium.random <-0l <-lm(MP ~ LLLT.random + Nicotine + Magnesium.random, data=llltRandom); summary(l); confint(l)# ...Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 3.28148626 0.06856553 47.85912 < 2e-16# LLLT.randomTRUE 0.04099628 0.09108322 0.45010 0.65324# NicotineTRUE 0.21152245 0.26673557 0.79300 0.42893# Magnesium.random 0.10299190 0.09312616 1.10594 0.27038## Residual standard error: 0.5809214 on 163 degrees of freedom# (47 observations deleted due to missingness)# Multiple R-squared: 0.01519483, Adjusted R-squared: -0.002930415# F-statistic: 0.8383241 on 3 and 163 DF, p-value: 0.474678## 2.5 % 97.5 %# (Intercept) 3.14609507948 3.4168774481# LLLT.randomTRUE -0.13885889747 0.2208514560# NicotineTRUE -0.31518017129 0.7382250752# Magnesium.random -0.08089731164 0.28688110340.04099628/sd(llltRandom$MP)# [1] 0.0701653002library(ggplot2)ggplot(data = llltRandom, aes(x=Date, y=MP, col=as.logical(llltRandom$LLLT.random))) +geom_point(size=I(3)) +stat_smooth() +scale_colour_manual(values=c("gray49", "blue"),name ="LLLT")
The estimate of the causal effect of LLLT+placebo is not statistically-significant, and the effect size of +0.04 / d = 0.07 is much smaller than d = 0.455 (15%) and the original pilot’s point estimate of +0.33 is excluded by the new confidence interval (95% CI: -0.13 - +0.22).
I have strong priors about the possible effects of LLLT, nicotine & magnesium (specifically, I know from experience that they tend to be small), so a Bayesian linear model using JAGS is useful for letting me take that into account and also producing more meaningful results (probabilities, rather than p-values):
## JAGS won't automatically drop rows with missing variables like `lm` does by defaultllltClean <- llltRandom[!is.na(llltRandom$LLLT.random),]library(rjags)library(R2jags)model1<-"model { for (i in 1:n) { MP[i] ~ dnorm(MP.hat[i], tau) MP.hat[i] <- a + b1*LLLT.random[i] + b2*Nicotine[i] + b3*Magnesium.random[i] } # intercept a ~ dnorm(3, 4) # precision 4 ~= 0.5^-2 ~= SD 0.5, the historical SD of my MPs # coefficients ## informative prior: effects should be <0.5 usually, and >0.3 is unusual b1 ~ dnorm(0, 13) # precision 13 ~= SD 0.3 b2 ~ dnorm(0, 13) b3 ~ dnorm(0, 13) # informative prior: 2-5 doesn't allow for much variance sigma ~ dunif(0, 1) # convert SD to 'precision' unit that JAGS's distributions use instead tau <- pow(sigma, -2)}"j1 <-with(llltClean, jags(data=list(n=nrow(llltClean), MP=MP, LLLT.random=LLLT.random,Nicotine=Nicotine, Magnesium.random=Magnesium.random),parameters.to.save=c("b1", "b2", "b3"),model.file=textConnection(model1),n.chains=getOption("mc.cores"), n.iter=1000000))print(j1, intervals=c(0.0001, 0.5, 0.9999))# Inference for Bugs model at "4", fit using jags,# 4 chains, each with 1e+06 iterations (first 5e+05 discarded), n.thin = 500# n.sims = 4000 iterations saved# mu.vect sd.vect 0.01% 50% 99.99% Rhat n.eff# b1 0.042 0.087 -0.276 0.041 0.326 1.002 2100# b2 0.114 0.194 -0.533 0.114 0.745 1.001 4000# b3 0.100 0.088 -0.266 0.100 0.412 1.001 4000# deviance 293.023 2.864 288.567 292.420 314.947 1.001 4000## For each parameter, n.eff is a crude measure of effective sample size,# and Rhat is the potential scale reduction factor (at convergence, Rhat=1).## DIC info (using the rule, pD = var(deviance)/2)# pD = 4.1 and DIC = 297.1# DIC is an estimate of expected predictive error (lower deviance is better).
This analysis suggests that there’s a 95% probability the effect is somewhere between -0.129 & 0.208 (d=-0.22 - d = 0.35), similar to the original linear model’s CI. More relevantly: there is only a 70% probability that the effect is >0 (albeit probably tiny), and >99.99% probability it’s not as big as the pilot data had claimed.
At small effects like d = 0.07, a nontrivial chance of negative effects, and an unknown level of placebo effects (this was non-blinded, which could account for any residual effects), this strongly implies that LLLT is not doing anything for me worth bothering with. I was pretty skeptical of LLLT in the first place, and if 167 days can’t turn up anything noticeable, I don’t think I’ll be continuing with LLLT usage and will be giving away my LED set. (Should any experimental studies of LLLT for cognitive enhancement in healthy people surface with large quantitative effects - as opposed to a handful of qualitative case studies about brain-damaged people - and I decide to give LLLT another try, I can always just buy another set of LEDs: it’s only ~$15, after all.)
See Melatonin for information on effects & cost; I regularly use melatonin to sleep (more to induce sleep than prolong or deepen it), and investigating with my Zeo, it does seem to improve & shorten my sleep. Some research suggests that higher doses are not necessarily better and may be overkill, so each time I’ve run out, I’ve been steadily decreasing the dose from 3mg to 1.5mg to 1mg, without apparently compromising the usefulness.
Here are the notes I jotted down while trying out modafinil back in November 200917ya. I didn’t make any effort to write sensibly, so this makes my lucidity seem much worse than it actually was:
Thursday: 3g piracetam/4g choline bitartrate at 1; 1 200mg modafinil at 2:20; noticed a ‘leveling’ of fatigue by 3:30; dry eyes? no bad after taste or anything. a little light-headed by 4:30, but mentally clear and focused. wonder if light-headedness is due simply to missing lunch and not modafinil. 5:43: noticed my foot jiggling - doesn’t usually jiggle while in piracetam/choline. 7:30: starting feeling a bit jittery & manic - not much or to a problematic level but definitely noticeable; but then, that often happens when I miss lunch & dinner. 12:30: bedtime. Can’t sleep even with 3mg of melatonin! Subjectively, I toss & turn (in part thanks to my cat) until 4:30, when I really wake up. I hang around bed for another hour & then give up & get up. After a shower, I feel fairly normal, strangely, though not as good as if I had truly slept 8 hours. The lesson here is to pay attention to wikipedia when it says the half-life is 12-15 hours! About 6AM I take 200mg; all the way up to 2pm I feel increasingly less energetic and unfocused, though when I do apply myself I think as well as ever. Not fixed by food or tea or piracetam/choline. I want to be up until midnight, so I take half a pill of 100mg and chew it (since I’m not planning on staying up all night and I want it to work relatively soon). From 4-12PM, I notice that today as well my heart rate is elevated; I measure it a few times and it seems to average to ~70BPM, which is higher than normal, but not high enough to concern me. I stay up to midnight fine, take 3mg of melatonin at 12:30, and have no trouble sleeping; I think I fall asleep around 1. Alarm goes off at 6, I get up at 7:15 and take the other 100mg. Only 100mg/half-a-pill because I don’t want to leave the half laying around in the open, and I’m curious whether 100mg + ~5 hours of sleep will be enough after the last 2 days. Maybe next weekend I’ll just go without sleep entirely to see what my limits are.
In general, I feel a little bit less alert, but still close to normal. By 6PM, I have a mild headache, but I try out 30 rounds of gbrainy (haven’t played it in months) and am surprised to find that I reach an all-time high; no idea whether this is due to DNB or not, since Gbrainy is very heavily ‘crystallized’ (half the challenge disappears as you learn how the problems work), but it does indicate I’m not deluding myself about mental ability. (To give a figure: my last score well before I did any DNB was 64, and I was doing well that day; on modafinil, I had a 77.) I figure the headache might be food related, eat, and by 7:30 the headache is pretty much gone and I’m fine up to midnight.
I took 1.5mg of melatonin, and went to bed at ~1:30AM; I woke up around 6:30, took a modafinil pill/200mg, and felt pretty reasonable. By noon my mind started to feel a bit fuzzy, and lunch didn’t make much of it go away. I’ve been looking at studies, and users seem to degrade after 30 hours; I started on mid-Thursday, so call that 10 hours, then 24 (Friday), 24 (Saturday), and 14 (Sunday), totaling 72hrs with <20hrs sleep; this might be equivalent to 52hrs with no sleep, and Wikipedia writes:
One study of helicopter pilots suggested that 600 mg of modafinil given in three doses can be used to keep pilots alert and maintain their accuracy at pre-deprivation levels for 40 hours without sleep.[60] However, significant levels of nausea and vertigo were observed. Another study of fighter pilots showed that modafinil given in three divided 100 mg doses sustained the flight control accuracy of sleep-deprived F-117 pilots to within about 27% of baseline levels for 37 hours, without any considerable side effects.[61] In an 88-hour sleep loss study of simulated military grounds operations, 400 mg⧸day doses were mildly helpful at maintaining alertness and performance of subjects compared to placebo, but the researchers concluded that this dose was not high enough to compensate for most of the effects of complete sleep loss.
If I stop tonight and do nothing Monday (and I sleep the normal eight hours and do not pay any penalty), then that’ll be 4 out of 5 days on modafinil, each saving 3 or 4 hours. Each day took one pill which cost me $1.20, but each pill saved let’s call it 3.5 hours; if I value my time at minimum wage, or 7.25/hr (federal minimum wage), then that 3.5 hours is worth $25.37, which is much more than $1.20, ~21x more.
My mental performance continues as before; curiously, I get an even higher score on Gbrainy, despite being sure I was less sharp than yesterday. Either I’m wrong about that, or Gbrainy is even more trainable than I thought. I go to bed Sunday around 1AM, and get up around 8AM (so call it 6 or 7 hours).
Monday: It’s a long day ahead of me, so I take 200mg. Reasonable performance.
Tuesday: I went to bed at 1am, and first woke up at 6am, and I wrote down a dream; the lucid dreaming book I was reading advised that waking up in the morning and then going back for a short nap often causes lucid dreams, so I tried that - and wound up waking up at 10am with no dreams at all. Oops. I take a pill, but the whole day I don’t feel so hot, although my conversation and arguments seem as cogent as ever. I’m also having a terrible time focusing on any actual work. At 8 I take another; I’m behind on too many things, and it looks like I need an all-nighter to catch up. The dose is no good; at 11, I still feel like at 8, possibly worse, and I take another along with the choline+piracetam (which makes a total of 600mg for the day). Come 12:30, and I disconsolately note that I don’t seem any better, although I still seem to understand the IQ essays I am reading. I wonder if this is tolerance to modafinil, or perhaps sleep catching up to me? Possibly it’s just that I don’t remember what the quasi-light-headedness of modafinil felt like. I feel this sort of zombie-like state without change to 4am, so it must be doing something, when I give up and go to bed, getting up at 7:30 without too much trouble. Some N-backing at 9am gives me some low scores but also some pretty high scores (38/43/66/40/24/67/60/71/54 or ▂▂▆▂▁▆▅▇▄), which suggests I can perform normally if I concentrate. I take another pill and am fine the rest of the day, going to bed at 1am as usual.
Thursday: this is an important day where I really need to be awake. I’m up around 8, take a pill, and save one for later; I’ll take half a pill at noon and the other half at 2. This works very well, and I don’t feel tired well up to midnight, even though I spent an hour walking.
Friday: alarm clock woke me at 7:40, but I somehow managed to go back to sleep until 9:40. Perhaps sleep inertia is building up despite the modafinil. Another pill. I am in general noticing less effect, but I’ll not take any this weekend to see whether I have simply gotten used to it.
Sat/Sun: bed at 1/2AM, awake at 10/11 respectively. Generally unmotivated.
Mon: went to bed at 11:30 Sun, woke at 7:30 and dozed to 8. 200mg at 8:30. No particular effect. Past this, I stop keeping notes. The main thing I notice is that my throat seems to be a little rough and my voice hoarser than usual.
(On a side note, I think I understand now why modafinil doesn’t lead to a Beggars in Spain scenario; BiS includes massive IQ and motivation boosts as part of the Sleepless modification. Just adding 8 hours a day doesn’t do the world-changing trick, no more than some researchers living to 90 and others to 60 has lead to the former taking over. If everyone were suddenly granted the ability to never need sleep, many of them would have no idea what to do with the extra 8 or 9 hours and might well be destroyed by the gift; it takes a lot of motivation to make good use of the time, and if one cannot, then it is a curse akin to the stories of immortals who yearn for death - they yearn because life is not a blessing to them, though that is a fact more about them than life.)
In 201115ya, as part of the Silk Road research, I ordered 10x100mg Modalert (5btc) from a seller. I also asked him about his sourcing, since if it was bad, it’d be valuable to me to know whether it was sourced from one of the vendors listed in my table. He replied, more or less, “I get them from a large Far Eastern pharmaceuticals wholesaler. I think they’re probably the supplier for a number of the online pharmacies.” 100mg seems likely to be too low, so I treated this shipment as 5 doses:
I split the 2 pills into 4 doses for each hour from midnight to 4 AM. 3D driver issues in Debian unstable prevented me from using Brain Workshop, so I don’t have any DNB scores to compare with the armodafinil DNB scores. I had the subjective impression that I was worse off with the Modalert, although I still managed to get a fair bit done so the deficits couldn’t’ve been too bad. The apathy during the morning felt worse than armodafinil, but that could have been caused by or exacerbated by an unexpected and very stressful 2 hour drive through rush hour and multiple accidents; the quick hour-long nap at 10 AM was half-waking half-light-sleep according to the Zeo, but seemed to help a bit. As before, I began to feel better in the afternoon and by evening felt normal, doing my usual reading. That night, the Zeo recorded my sleep as lasting ~9:40, when it was usually more like 8:40-9:00 (although I am not sure that this was due to the modafinil inasmuch as once a week or so I tend to sleep in that long, as I did a few days later without any influence from the modafinil); assuming the worse, the nap and extra sleep cost me 2 hours for a net profit of ~7 hours. While it’s not clear how modafinil affects recovery sleep (see the footnote in the essay), it’s still interesting to ponder the benefits of merely being able to delay sleep20.
I tried taking whole pills at 1 and 3 AM. I felt kind of bushed at 9 AM after all the reading, and the 50 minute nap didn’t help much - I was sleep only around 10 minutes and spent most of it thinking or meditation. Just as well the 3D driver is still broken; I doubt the scores would be reasonable. Began to perk up again past 10 AM, then felt more bushed at 1 PM, and so on throughout the day; kind of gave up and began watching & finishing anime (Amagami and Voices of a Distant Star) for the rest of the day with occasional reading breaks (eg. to start James C. Scott’sSeeing Like A State, which is as described so far). As expected from the low quality of the day, the recovery sleep was bigger than before: a full 10 hours rather than 9:40; the next day, I slept a normal 8:50, and the following day ~8:20 (woken up early); 10:20 (slept in); 8:44; 8:18 (▁▇▁▁). It will be interesting to see whether my excess sleep remains in the hour range for ‘good’ modafinil nights and two hours for ‘bad’ modafinil nights.
I decided to try out day-time usage on 2 consecutive days, taking the 100mg at noon or 1 PM. On both days, I thought I did feel more energetic but nothing extraordinary (maybe not even as strong as the nicotine), and I had trouble falling asleep on Halloween, thinking about the meta-ethics essay I had been writing diligently on both days. Not a good use compared to staying up a night.
Most people I talk to about modafinil seem to use it for daytime usage; for me that has not ever worked out well, but I had nothing in particular to show against it. So, as I was capping the last of my piracetam-caffeine mix and clearing off my desk, I put the 4 remaining Modalerts pills into capsules with the last of my creatine powder and then mixed them with 4 of the theanine-creatine pills. Like the previous Adderall trial, I will pick one pill blindly each day and guess at the end which it was. If it was active (modafinil-creatine), take a break the next day; if placebo (theanine-creatine), replace the placebo and try again the next day. We’ll see if I notice anything on DNB or possibly Gwern.net edits.
Take at 10 AM; seem a bit more active but that could just be the pressure of the holiday season combined with my nice clean desk. I do the chores without too much issue and make progress on other things, but nothing major; I survive going to The Sitter without too much tiredness, so ultimately I decide to give the palm to it being active, but only with 60% confidence. I check the next day, and it was placebo. Oops.
Take at 11 AM; distractions ensue and the Christmas tree-cutting also takes up much of the day. By 7 PM, I am exhausted and in a bad mood. While I don’t expect day-time modafinil to buoy me up, I do expect it to at least buffer me against being tired, and so I conclude placebo this time, and with more confidence than yesterday (65%). I check before bed, and it was placebo.
10:30 AM; no major effect that I notice throughout the day - it’s neither good nor bad. This smells like placebo (and part of my mind is going ‘how unlikely is it to get placebo 3 times in a row!’, which is just the Gambler’s fallacy talking inasmuch as this is sampling with replacement). I give it 60% placebo; I check the next day right before taking, and it is. Man!
1 PM; overall this was a pretty productive day, but I can’t say it was very productive. I would almost say even odds, but for some reason I feel a little more inclined towards modafinil. Say 55%. That night’s sleep was vile: the Zeo says it took me 40 minutes to fall asleep, I only slept 7:37 total, and I woke up 7 times. I’m comfortable taking this as evidence of modafinil (half-life 10 hours, 1 PM to midnight is only 1 full halving), bumping my prediction to 75%. I check, and sure enough - modafinil.
10:40 AM; again no major effects, although I got two jQuery extensions working and some additional writing so one could argue the day went well. I don’t know; 50%. Placebo.
11 AM; a rather productive day. I give it 65%. To my surprise, it was placebo.
10 AM; this was an especially productive day, but this was also the day my nicotine gum finally arrived and I just had to try it (I had been waiting so long); it’s definitely a stimulant, alright. But this trashes my own subjective estimates; I hoped it was just placebo, but no, it was modafinil.
9:50 AM; nothing noticed by noon. Managed to finish “Reasons of State: Why Didn’t Denmark Sell Greenland?” which was a surprising amount of work, especially after I managed to delete a third of the first draft - but nothing I would chalk up to modafinil. I decide to give it 60% placebo, and I turn out to be wrong: it was my last modafinil.
So with these 8 results in hand, what do I think? Roughly, I was right 5 of the days and wrong 3 of them. If not for the sleep effect on #4, which is - in a way - cheating (one hopes to detect modafinil due to good effects), the ratio would be 5:4 which is awfully close to a coin-flip. Indeed, a scoring rule ranks my performance at almost identical to a coin flip: -5.49 vs -5.5421. (The bright side is that I didn’t do worse than a coin flip: I was at least calibrated.)
I can’t call this much of a success; there may be an effect on my productivity but it’s certainly not very clear subjectively. I’ll chalk this up as a failure for modafinil and evidence for what I believed - day-time modafinil use does not work for me (even if it works for others).
For background on “value of information” calculations, see the Adderall calculation.
I had tried 8 randomized days like the Adderall experiment to see whether I was one of the people whom modafinil energizes during the day. (The other way to use it is to skip sleep, which is my preferred use.) I rarely use it during the day since my initial uses did not impress me subjectively. The experiment was not my best - while it was double-blind randomized, the measurements were subjective, and not a good measure of mental functioning like dual n-back (DNB) scores which I could statistically compare from day to day or against my many previous days of dual n-back scores. Between my high expectation of finding the null result, the poor experiment quality, and the minimal effect it had (eliminating an already rare use), the value of this information was very small.
I mostly did it so I could tell people that “no, day usage isn’t particularly great for me; why don’t you run an experiment on yourself and see whether it was just a placebo effect (or whether you genuinely are sleep-deprived and it is indeed compensating)?”
Besides Adderall, I also purchased on Silk Road 5x250mg pills of armodafinil. The price was extremely reasonable, 1.5btc or roughly $23 at that day’s exchange rate; I attribute the low price to the seller being new and needing feedback, and offering a discount to induce buyers to take a risk on him. (Buyers bear a large risk on Silk Road since sellers can easily physically anonymize themselves from their shipment, but a buyer can be found just by following the package.) Because of the longer active-time, I resolved to test the armodafinil not during the day, but with an all-nighter.
Took full pill at 10:21 PM when I started feeling a bit tired. Around 11:30, I noticed my head feeling fuzzy but my reading seemed to still be up to snuff. I would eventually finish the science book around 9 AM the next day, taking some very long breaks to walk the dog, write some poems, write a program, do Mnemosyne review (memory performance: subjectively below average, but not as bad as I would have expected from staying up all night), and some other things. Around 4 AM, I reflected that I felt much as I had during my nightwatch job at the same hour of the day - except I had switched sleep schedules for the job. The tiredness continued to build and my willpower weakened so the morning wasn’t as productive as it could have been - but my actual performance when I could be bothered was still pretty normal. That struck me as kind of interesting that I can feel very tired and not act tired, in line with the anecdotes.
Past noon, I began to feel better, but since I would be driving to errands around 4 PM, I decided to not risk it and take an hour-long nap, which went well, as did the driving. The evening was normal enough that I forgot I had stayed up the previous night, and indeed, I didn’t much feel like going to bed until past midnight. I then slept well, the Zeo giving me a 108 ZQ (not an all-time record, but still unusual).
I had intended to run another Adderall trial this day but then I learned we would be going to the midnight showing of the last Harry Potter movie. A perfect opportunity: going to bed at 3 AM after a stimulating battle movie would mean crappy sleep, so why not just do another armodafinil trial and kill 2 birds with one stone?
I took the pill at 11 PM the evening of (technically, the day before); that day was a little low on sleep than usual, since I had woken up an hour or half-hour early. I didn’t yawn at all during the movie (merely mediocre to my eyes with some questionable parts)24. It worked much the same as it did the previous time - as I walked around at 5 AM or so, I felt perfectly alert. I made good use of the hours and wrote up some stuff.
(As I was doing this, I reflected how modafinil is such a pure example of the money-time tradeoff. It’s not that you pay someone else to do something for you, which necessarily they will do in a way different from you; nor is it that you have exchanged money to free yourself of a burden of some future time-investment; nor have you paid money for a speculative return of time later in life like with many medical expenses or supplements. Rather, you have paid for 8 hours today of your own time.)
And as before, around 9 AM I began to feel the peculiar feeling that I was mentally able and apathetic (in a sort of aboulia way); so I decided to try what helped last time, a short nap. But this time, though I took a full hour, I slept not a wink and my Zeo recorded only 2 transient episodes of light sleep! A back-handed sort of proof of alertness, I suppose. I didn’t bother trying again. The rest of the day was mediocre, and I wound up spending much of it on chores and whatnot out of my control. Mentally, I felt better past 3 PM.
This continued up to 1 AM, at which point I decided not to take a second armodafinil (why spend a second pill to gain what would likely be an unproductive set of 8 hours?) and finish up the experiment with some n-backing. My 5 rounds: 60/38/62/44/5025. This was surprising. Compare those scores with scores from several previous days: 39/42/44/40/20/28/36. I had estimated before the n-backing that my scores would be in the low-end of my usual performance (20-30%) since I had not slept for the past 41 hours, and instead, the lowest score was 38%. If one did not know the context, one might think I had discovered a good nootropic! Interesting evidence that armodafinil preserves at least one kind of mental performance.
I stayed up late writing some poems and about how Folding@home kills, and decided to make a night of it. I took the armodafinil at 1 AM; the interesting bit is that this was the morning/evening after what turned out to be an Adderall (as opposed to placebo) trial, so perhaps I will see how well or ill they go together. A set of normal scores from a previous day was 32%/43%/51%/48%. At 11 PM, I scored 39% on DNB; at 1 AM, I scored 50%/43%; 5:15 AM, 39%/37%; 4:10 PM, 42%/40%; 11 PM, 55%/21%/38%. (▂▄▆▅ vs ▃▅▄▃▃▄▃▇▁▃)
The peculiar tired-sharp feeling was there as usual, and the DNB scores continue to suggest this is not an illusion, as they remain in the same 30-50% band as my normal performance. I did not notice the previous ‘aboulia’ feeling; instead, around noon, I was filled with a nervous energy and a disturbingly rapid pulse which meditation & deep breathing did little to help with, and which didn’t go away for an hour or so. Fortunately, this was primarily at church, so while I felt irritable, I didn’t actually interact with anyone or snap at them, and was able to keep a lid on it. I have no idea what that was about. I wondered if it might’ve been a serotonin storm since amphetamines are some of the drugs that can trigger storms but the Adderall had been at 10:50 AM the previous day, or >25 hours (the half-lives of the ingredients being around 13 hours). An hour or two previously I had taken my usual caffeine-piracetam pill with my morning tea - could that have interacted with the armodafinil and the residual Adderall? Or was it caffeine+modafinil? Speculation, perhaps. A house-mate was ill for a few hours the previous day, so maybe the truth is as prosaic as me catching whatever he had.
Stayed up with the purpose of finishing my work for a contest. This time, instead of taking the pill as a single large dose (I feel that after 3 times, I understand what it’s like), I will take 4 doses over the new day. I took the first quarter at 1 AM, when I was starting to feel a little foggy but not majorly impaired. Second dose, 5:30 AM; feeling a little impaired. 8:20 AM, third dose; as usual, I feel physically a bit off and mentally tired - but still mentally sharp when I actually do something. Early on, my heart rate seemed a bit high and my limbs trembling, but it’s pretty clear now that that was the caffeine or piracetam. It may be that the other day, it was the caffeine’s fault as I suspected. The final dose was around noon. The afternoon ‘crash’ wasn’t so pronounced this time, although motivation remains a problem. I put everything into finishing up the spaced repetition literature review, and didn’t do any n-backing until 11:30 PM: 32/34/31/54/40%.
With the last pill, I wound up trying split-doses on non-full nights; that is, if one full pill keeps me awake one full night, what does 1/4th the pill do?
Between midnight and 1:36 AM, I do four rounds of n-back: 50/39/30/55%. I then take 1/4th of the pill and have some tea. At roughly 1:30 AM, AngryParsley linked a SF anthology/novel, Fine Structure, which sucked me in for the next 3-4 hours until I finally finished the whole thing. At 5:20 AM, circumstances forced me to go to bed, still having only taken 1/4th of the pill and that determines this particular experiment of sleep; I quickly do some n-back: 29/20/20/54/42. I fall asleep in 13 minutes and sleep for 2:48, for a ZQ of 28 (a full night being ~100). I did not notice anything from that possible modafinil+caffeine interaction. Subjectively upon awakening: I don’t feel great, but I don’t feel like 2-3 hours of sleep either. N-back at 10 AM after breakfast: 25/54/44/38/33. These are not very impressive, but seem normal despite taking the last armodafinil ~9 hours ago; perhaps the 3 hours were enough. Later that day, at 11:30 PM (just before bed): 26/56/47.
2 break days later, I took the quarter-pill at 11:22 PM. I had discovered I had for years physically possessed a very long interview not available online, and transcribing that seemed like a good way to use up a few hours. I did some reading, some Mnemosyne, and started it around midnight, finishing around 2:30 AM. There seemed a mental dip around 30 minutes after the armodafinil, but then things really picked up and I made very good progress transcribing the final draft of 9000 words in that period. (In comparison, “The Conscience of the Otaking” parts 2 & 4 were much easier to read than the tiny font of the RahXephon booklet, took perhaps 3 hours, and totaled only 6500 words. The nicotine is probably also to thank.) By 3:40 AM, my writing seems to be clumsier and my mind fogged. Began DNB at 3:50: 61/53/44. Went to bed at 4:05, fell asleep in 16 minutes, slept for 3:56. Waking up was easier and I felt better, so the extra hour seemed to help.
With this experiment, I broke from the previous methodology, taking the remaining and final half Nuvigil at midnight. I am behind on work and could use a full night to catch up. By 8 AM, I am as usual impressed by the Nuvigil - with Modalert or something, I generally start to feel down by mid-morning, but with Nuvigil, I feel pretty much as I did at 1 AM. Sleep: 9:51/9:15/8:27
I noticed on SR something I had never seen before, an offer for 150mgx10 of “Waklert” for ₿13.47 (then, ₿1 = $3.14). I searched and it seemed Sun was somehow manufacturing armodafinil! Interesting. Maybe not cost-effective, but I tried out of curiosity. They look and are packaged the same as the Modalert, but at a higher price-point: 150 rather than 81 rupees. Not entirely sure how to use them: assuming quality is the same, 150mg Waklert is still 100mg less armodafinil than the 250mg Nuvigil pills.
Take quarter at midnight, another quarter at 2 AM. Night runs reasonably well once I remember to eat a lot of food (I finish a big editing task I had put off for weeks), but the apathy kicks in early around 4 AM so I gave up and watched Scott Pilgrim versus the World, finishing around 6 AM. I then read until it’s time to go to a big shotgun club function, which occupies the rest of the morning and afternoon; I had nothing to do much of the time and napped very poorly on occasion. By the time we got back at 4 PM, the apathy was completely gone and I started some modafinil research with gusto (interrupted by going to see Puss in Boots). That night: Zeo recorded 8:30 of sleep, gap of about 1:50 in the recording, figure 10:10 total sleep; following night, 8:33; third night, 8:47; fourth, 8:20 (▇▁▁▁).
First quarter at 1:20 AM. Second quarter at 4 AM. 20 minute nap at 7:30 AM; took show and last 2 doses at 11 AM. (If I feel bad past 3 PM, I’ll try one of the Modalerts or maybe another quarter of a Waklert - 150mg may just be too little.) Overall, pretty good day. Nights: 9:43; 9:51; 7:57; 8:25; 8:08; 9:02; 8:07 (▇█▁▂▁▄▁).
First half at 6 AM; second half at noon. Wrote a short essay I’d been putting off and napped for 1:40 from 9 AM to 10:40. This approach seems to work a little better as far as the aboulia goes. (I also bother to smell my urine this time around - there’s a definite off smell to it.) Nights: 10:02; 8:50; 10:40; 7:38 (2 bad nights of nasal infections); 8:28; 8:20; 8:43 (▆▃█▁▂▂▃).
Whole pill at 5:42 AM. (Somewhat productive night/morning beforehand.) DNB at 2 PM: 52/36/54 (▇▁█); slept for 49 minutes; DNB at 8 PM: 50/44/38/40 (▆▄▁▂). Nights: 10:02; 8:02; no data; 9:21; 8:20 (█▁ ▅▂).
Whole pill at 3 AM. I spend the entire morning and afternoon typing up a transcript of “Earth in My Window”. I tried taking a nap around 10 AM, but during the hour I was down, I had <5m of light sleep, the Zeo said. After I finished the transcript (~16,600 words with formatting), I was completely pooped and watched a bunch of Mobile Suit Gundam episodes, then I did Mnemosyne. The rest of the night was nothing to write home about either - some reading, movie watching, etc. Next time I will go back to split-doses and avoid typing up 110kB of text. On the positive side, this is the first trial I had available the ‘average daily grade’ Mnemosyne 2.0 plugin. The daily averages all are 3-point-something (peaking at 3.89 and flooring at 3.59), so just graphing the past 2 weeks, the modafinil day, and recovery days: ▅█▅▆▄▆▄▃▅▄▁▄▄ ▁ ▂▄▄█. Not an impressive performance but there was a previous non-modafinil day just as bad, and I’m not too sure how important a metric this is; I must see whether future trials show similar underperformance. Nights: 11:29; 9:22; 8:25; 8:41.
Spaced repetition at midnight: 3.68. (Graphing preceding and following days: ▅▄▆▆▁▅▆▃▆▄█ ▄ ▂▄▄▅) DNB starting 12:55 AM: 30/34/41. Transcribed Sawaragi 2005, then took a walk. DNB starting 6:45 AM: 45/44/33. Decided to take a nap and then take half the armodafinil on awakening, before breakfast. I wound up oversleeping until noon (4:28); since it was so late, I took only half the armodafinil sublingually. I spent the afternoon learning how to do “value of information” calculations, and then carefully working through 8 or 9 examples for my various pages, which I published on Lesswrong. That was a useful little project. DNB starting 12:09 AM: 30/38/48. (To graph the preceding day and this night: ▇▂█▆▅▃▃▇▇▇▁▂▄ ▅▅▁▁▃▆) Nights: 9:13; 7:24; 9:13; 8:20; 8:31.
Feeling behind, I resolved to take some armodafinil the next morning, which I did - but in my hurry I failed to recall that 200mg armodafinil was probably too much to take during the day, with its long half life. As a result, I felt irritated and not that great during the day (possibly aggravated by some caffeine - I wish some studies would be done on the possible interaction of modafinil and caffeine so I knew if I was imagining it or not). Certainly not what I had been hoping for. I went to bed after midnight (half an hour later than usual), and suffered severe insomnia. The time wasn’t entirely wasted as I wrote a short story and figured out how to make nicotine gum placebos during the hours in the dark, but I could have done without the experience. All metrics omitted because it was a day usage.
NGF may sound intriguing, but the price is a dealbreaker: at suggested doses of 1-100μg (NGF dosing in humans for benefits is, shall we say, not an exact science), and a cost from sketchy suppliers of $1,210/100μg/$470/500μg/$750/1000μg/$1,000/1000μg/$1,030/1000μg/$235/20μg. (Levi-Montalcini was presumably able to divert some of her lab’s production.) A year’s supply then would be comically expensive: at the lowest doses of 1-10μg using the cheapest sellers (for something one is dumping into one’s eyes?), it could cost anywhere up to $10,000.
As well, the possible effects seem like they would be long-term and difficult to measure or experiment on; so if one could somehow afford NGF eyedrops, one wouldn’t be able to know they were working.
So unless the price of NGF comes down by at least two orders of magnitude, it’s not a viable nootropic.
One of the most popular legal stimulants in the world, nicotine is often conflated with the harmful effects of tobacco; considered on its own, it has performance & possibly health benefits. Nicotine is widely available at moderate prices as long-acting nicotine patches, gums, lozenges, and suspended in water for vaping. While intended for smoking cessation, there is no reason one cannot use a nicotine patch or nicotine gum for its stimulant effects.
Nicotine’s stimulant effects are general and do not come with the same tweakiness and aggression associated with the amphetamines, and subjectively are much ‘cleaner’ with less of a crash. I would say that its stimulant effects are fairly strong, around that of modafinil. Another advantage is that nicotine operates through nicotinic receptors and so doesn’t cross-tolerate with dopaminergic stimulants (hence one could hypothetically cycle through nicotine, modafinil, amphetamines, and caffeine, hitting different receptors each time).
Like caffeine, nicotine tolerates rapidly and addiction can develop, after which the apparent performance boosts may only represent a return to baseline after withdrawal; so nicotine as a stimulant should be used judiciously, perhaps roughly as frequent as modafinil. Another problem is that nicotine has a half-life of merely 1-2 hours, making regular dosing a requirement. There is also some elevated heart-rate/blood-pressure often associated with nicotine, which may be a concern. (Possible alternatives to nicotine include cytisine, 2’-methylnicotine, GTS-21, galantamine, Varenicline, WAY-317,538, EVP-6124, and Wellbutrin, but none have emerged as clearly superior.)
I decided to try it out myself since it would be both boring and hypocritical not to. The stimulant properties are well-established, and after reading up, I didn’t think there was a >3% chance it might lead me to any short or long-term future cigarette use.
So I ordered the most cost-effective batch of chewing gum I could find on Amazon (100 Nicorette 4mg) - and the seller canceled on me! Poor show, “Direct Super center”, very poor show.
In August 201115ya, after winning the spaced repetition contest and finishing up the Adderall double-blind testing, I decided the time was right to try nicotine again. I had since learned that e-cigarettes use nicotine dissolved in water, and that nicotine-water was a vastly cheaper source of nicotine than either gum or patches. So I ordered 250ml of water at 12mg/ml (total cost: $18.20). A cigarette apparently delivers around 1mg of nicotine, so half a ml would be a solid dose of nicotine, making that ~500 doses. Plenty to experiment with. The question is, besides the stimulant effect, nicotine also causes ‘habit formation’; what habits should I reinforce with nicotine? Exercise, and spaced repetition seem like 2 good targets.
It arrived as described, a little bottle around the volume of a soda can. I had handy a plastic syringe with milliliter units which I used to measure out the nicotine-water into my tea. I began with half a ml the first day, 1ml the second day, and 2ml the third day. (My Zeo sleep scores were 85/103/86 (▁▇▁), and the latter had a feline explanation; these values are within normal variation for me, so if nicotine affects my sleep, it does so to a lesser extent than Adderall.) Subjectively, it’s hard to describe. At half a ml, I didn’t really notice anything; at 1 and 2ml, I thought I began to notice it - sort of a cleaner caffeine. It’s nice so far. It’s not as strong as I expected. I looked into whether the boiling water might be breaking it down, but the answer seems to be no - boiling tobacco is a standard way to extract nicotine, actually, and nicotine’s own boiling point is much higher than water; nor do I notice a drastic difference when I take it in ordinary water. And according to various e-cigarette sources, the liquid should be good for at least a year.
2ml is supposed to translate to 24mg, which is a big dose. I do not believe any of the commercial patches go much past that. I asked Wedrifid, whose notes inspired my initial interest, and he was taking perhaps 2-4mg, and expressed astonishment that I might be taking 24mg. (2mg is in line with what I am told by another person - that 2mg was so much that they actually felt a little sick. On the other hand, in one study, the subjects could not reliably distinguish between 1mg and placebo26.) 24mg is particularly troubling in that I weigh ~68kg, and nicotine poisoning and the nicotine LD50 start, for me, at around 68mg of nicotine. (I reflected that the entire jar could be a useful murder weapon, although nicotine presumably would be caught in an autopsy’s toxicology screen; I later learned nicotine was an infamous weapon in the 1800s before any test was developed. It doesn’t seem used anymore, but there are still fatal accidents due to dissolved nicotine.) The upper end of the range, 10mg⧸kg or 680mg for me, is calculated based on experienced smokers. Something is wrong here - I can’t see why I would have nicotine tolerance comparable to a hardened smoker, inasmuch as my maximum prior exposure was second-hand smoke once in a blue moon. More likely is that either the syringe is misleading me or the seller NicVape sold me something more dilute than 12mg/ml. (I am sure that it’s not simply plain water; when I mix the drops with regular water, I can feel the propylene glycol burning as it goes down.) I would rather not accuse an established and apparently well-liked supplier of fraud, nor would I like to simply shrug and say I have a mysterious tolerance and must experiment with doses closer to the LD50, so the most likely problem is a problem with the syringe. The next day I altered the procedure to sucking up 8ml, squirting out enough fluid to move the meniscus down to 7ml, and then ejecting the rest back into the container. The result was another mild clean stimulation comparable to the previous 1ml days. The next step is to try a completely different measuring device, which doesn’t change either.
One item always of interest to me is sleep; a stimulant is no good if it damages my sleep (unless that’s what it is supposed to do, like modafinil) - anecdotesandresearch suggest that it does. Over the past few days, my Zeo sleep scores continued to look normal. But that was while not taking nicotine much later than 5 PM. In lieu of a different ml measurer to test my theory that my syringe is misleading me, I decide to more directly test nicotine’s effect on sleep by taking 2ml at 10:30 PM, and go to bed at 12:20; I get a decent ZQ of 94 and I fall asleep in 16 minutes, a bit below my weekly average of 19 minutes. The next day, I take 1ml directly before going to sleep at 12:20; the ZQ is 95 and time to sleep is 14 minutes.
The next cheap proposition to test is that the 2ml dose is so large that the sedation/depressive effect of nicotine has begun to kick in. This is easy to test: take much less, like half a ml. I do so two or three times over the next day, and subjectively the feeling seems to be the same - which seems to support that proposition (although perhaps I’ve been placebo effecting myself this whole time, in which case the exact amount doesn’t matter). If this theory is true, my previous sleep results don’t show anything; one would expect nicotine-as-sedative to not hurt sleep or improve it. I skip the day (no cravings or addiction noticed), and take half a ml right before bed at 11:30; I fall asleep in 12 minutes and have a ZQ of ~105. The next few days I try putting one or two drops into the tea kettle, which seems to work as well (or poorly) as before. At that point, I was warned that there were some results that nicotine withdrawal can kick in with delays as long as a week, so I shouldn’t be confident that a few days off proved an absence of addiction; I immediately quit to see what the week would bring. 4 or 7 days in, I didn’t notice anything. I’m still using it, but I’m definitely a little nonplussed and disgruntled - I need some independent source of nicotine to compare with!
After trying the nicotine gum (see below) and experiencing effects, I decided the liquid was busted somehow and to request a refund. To its credit, NicVape immediately agreed to a refund.
2 commenters point out that my possible lack of result is due to my mistaken assumption that if nicotine is absorbable through skin, mouth, and lungs it ought to be perfectly fine to absorb it through my stomach by drinking it (rather than vaporizing it and breathing it with an e-cigarette machine) - it’s apparently known that absorption differs in the stomach.
the online book The Cigarette Papers describes early animal experiments (without specific bioavailability percentages):
…The Fate of Nicotine in the Body also describes Battelle’s animal work on nicotine absorption. Using C14-labeled nicotine in rabbits, the Battelle scientists compared gastric absorption with pulmonary absorption. Gastric absorption was slow, and first pass removal of nicotine by the liver (which transforms nicotine into inactive metabolites) was demonstrated following gastric administration, with consequently low systemic nicotine levels. In contrast, absorption from the lungs was rapid and led to widespread distribution. These results show that nicotine absorbed from the stomach is largely metabolized by the liver before it has a chance to get to the brain. That is why tobacco products have to be puffed, smoked or sucked on, or absorbed directly into the bloodstream (ie. via a nicotine patch). A nicotine pill would not work because the nicotine would be inactivated before it reached the brain.
Absorption of nicotine across biological membranes depends on pH. Nicotine is a weak base with a pKa of 8.0 (Fowler, 195472ya). In its ionized state, such as in acidic environments, nicotine does not rapidly cross membranes…About 80 to 90% of inhaled nicotine is absorbed during smoking as assessed using C14-nicotine (Armitage et al 197551ya). The efficacy of absorption of nicotine from environmental smoke in nonsmoking women has been measured to be 60 to 80% (Iwase et al 199135ya)…The various formulations of nicotine replacement therapy (NRT), such as nicotine gum, transdermal patch, nasal spray, inhaler, sublingual tablets, and lozenges, are buffered to alkaline pH to facilitate the absorption of nicotine through cell membranes. Absorption of nicotine from all NRTs is slower and the increase in nicotine blood levels more gradual than from smoking (Table 1). This slow increase in blood and especially brain levels results in low abuse liability of NRTs (Henningfield and Keenan, 199333ya; West et al 200026ya). Only nasal spray provides a rapid delivery of nicotine that is closer to the rate of nicotine delivery achieved with smoking (Sutherland et al 199234ya; Gourlay and Benowitz, 199729ya; Guthrie et al 199927ya). The absolute dose of nicotine absorbed systemically from nicotine gum is much less than the nicotine content of the gum, in part, because considerable nicotine is swallowed with subsequent first-pass metabolism (Benowitz et al 198739ya). Some nicotine is also retained in chewed gum. A portion of the nicotine dose is swallowed and subjected to first-pass metabolism when using other NRTs, inhaler, sublingual tablets, nasal spray, and lozenges (Johansson et al 199135ya; Bergstrom et al 199531ya; Lunell et al 199630ya; Molander and Lunell, 200125ya; Choi et al 200323ya). Bioavailability for these products with absorption mainly through the mucosa of the oral cavity and a considerable swallowed portion is about 50 to 80% (Table 1)…Nicotine is poorly absorbed from the stomach because it is protonated (ionized) in the acidic gastric fluid, but is well absorbed in the small intestine, which has a more alkaline pH and a large surface area. Following the administration of nicotine capsules or nicotine in solution, peak concentrations are reached in about 1 h (Benowitz et al 199135ya; Zins et al 199729ya; Dempsey et al 200422ya). The oral bioavailability of nicotine is about 20 to 45% (Benowitz et al 199135ya; Compton et al 199729ya; Zins et al 199729ya). Oral bioavailability is incomplete because of the hepatic first-pass metabolism. Also the bioavailability after colonic (enema) administration of nicotine (examined as a potential therapy for ulcerative colitis) is low, around 15 to 25%, presumably due to hepatic first-pass metabolism (Zins et al 199729ya). Cotinine is much more polar than nicotine, is metabolized more slowly, and undergoes little, if any, first-pass metabolism after oral dosing (Benowitz et al 198343yab; De Schepper et al 198739ya; Zevin et al 199729ya).
Nicotine was well absorbed, mean 18.6±3.4% in 15 min, on intragastric instillation at pH 9.8. Absorption was accompanied by side effects of nausea and vomiting, and delay in gastric emptying. Gastric absorption of nicotine at pH 7.4 was less marked (mean 8.2±2.9%), but was negligible at pH 1 (mean 3.3±1.4%).
Nicotine absorption through the stomach is variable and relatively reduced in comparison with absorption via the buccal cavity and the small intestine. ‘Drinking’, ‘eating’, and swallowing of tobacco smoke by South American Indians have frequently been reported. Tenetehara shamans reach a state of tobacco narcosis through large swallows of smoke, and Tapirape shams are said to “eat smoke” by forcing down large gulps of smoke only to expel it again in a rapid sequence of belches. In general, swallowing of tobacco smoke is quite frequently likened to ‘drinking’. However, although the amounts of nicotine swallowed in this way - or in the form of saturated saliva or pipe juice - may be large enough to be behaviorally significant at normal levels of gastric pH, nicotine, like other weak bases, is not significantly absorbed.
From the standpoint of absorption, the drinking of tobacco juice and the interaction of the infusion or concoction with the small intestine is a highly effective method of gastrointestinal nicotine administration. The epithelial area of the intestines is incomparably larger than the mucosa of the upper tract including the stomach, and “the small intestine represents the area with the greatest capacity for absorption” (Levine 198343ya:81-83). As practiced by most of the sixty-four tribes documented here, intoxicated states are achieved by drinking tobacco juice through the mouth and/or nose…The large intestine, although functionally little equipped for absorption, nevertheless absorbs nicotine that may have passed through the small intestine.
It looks like the overall picture is that nicotine is absorbed well in the intestines and the colon, but not so well in the stomach; this might be the explanation for the lack of effect, except on the other hand, the specific estimates I see are that 10-20% of the nicotine will be bioavailable in the stomach (as compared to 50%+ for mouth or lungs)… so any of my doses of >5ml should have overcome the poorer bioavailability! But on the gripping hand, these papers are mentioning something about the liver metabolizing nicotine when absorbed through the stomach, so…
So I eventually got around to ordering another thing of nicotine gum, “Habitrol Nicotine Gum, 4mg MINT flavor COATED gum. 96 pieces per box”. Gum should be easier to double-blind myself with than nicotine patches - just buy some mint gum. If 4mg is too much, cut the gum in half or whatever. When it arrived, my hopes were borne out: the gum was rectangular and soft, which made it easy to cut into fourths.
Remembering what Wedrifid told me, I decided to start with a quarter of a piece (~1mg). The gum was pretty tasteless, which ought to make blinding easier. The effects were noticeable around 10 minutes - greater energy verging on jitteriness, much faster typing, and apparent general quickening of thought. Like a more pleasant caffeine. While testing my typing speed in Amphetype, my speed seemed to go up >=5 WPM, even after the time penalties for correcting the increased mistakes; I also did twice the usual number without feeling especially tired. A second dose was similar, and the third dose was at 10 PM before playing Ninja Gaiden II seemed to stop the usual exhaustion I feel after playing through a level or so. (It’s a tough game, which I have yet to master like Ninja Gaiden Black.) Returning to the previous concern about sleep problems, though I went to bed at 11:45 PM, it still took 28 minutes to fall sleep (compared to my more usual 10-20 minute range); the next day I use 2mg from 7-8PM while driving, going to bed at midnight, where my sleep latency is a more reasonable 14 minutes. I then skipped for 3 days to see whether any cravings would pop up (they didn’t). I subsequently used 1mg every few days for driving or Ninja Gaiden II, and while there were no cravings or other side-effects, the stimulation definitely seemed to get weaker - benefits seemed to still exist, but I could no longer describe any considerable energy or jitteriness.
The easiest way to use 2mg was to use half a gum; I tried not chewing it but just holding it in my cheek. The first night I tried, this seemed to work well for motivation; I knocked off a few long-standing to-do items. Subsequently, I began using it for writing, where it has been similarly useful. One difficult night, I wound up using the other half (for a total of 4mg over ~5 hours), and it worked but gave me a fairly mild headache and a faint sensation of nausea; these may have been due to forgetting to eat dinner, but this still indicates 3mg should probably be my personal ceiling until and unless tolerance to lower doses sets in.
Blinding stymied me for a few months since the nasty taste was unmistakable and I couldn’t think of any gums with a similar flavor to serve as placebo. (The nasty taste does not seem to be due to the nicotine despite what one might expect; Vaniver plausibly suggested the bad taste might be intended to prevent over-consumption, but nothing in the Habitrol ingredient list seemed to be noted for its bad taste, and a number of ingredients were sweetening sugars of various sorts. So I couldn’t simply flavor some gum.)
I almost resigned myself to buying patches to cut (and let the nicotine evaporate) and hope they would still stick on well enough afterwards to be indistinguishable from a fresh patch, when late one sleepless night I realized that a piece of nicotine gum hanging around on my desktop for a week proved useless when I tried it, and that was the answer: if nicotine evaporates from patches, then it must evaporate from gum as well, and if gum does evaporate, then to make a perfect placebo all I had to do was cut some gum into proper sizes and let the pieces sit out for a while. (A while later, I lost a piece of gum overnight and consumed the full 4mg to no subjective effect.) Google searches led to nothing indicating I might be fooling myself, and suggested that evaporation started within minutes in patches and a patch was useless within a day. Just a day is pushing it (who knows how much is left in a useless patch?), so I decided to build in a very large safety factor and let the gum sit for around a month rather than a single day.
The experiment then is straightforward: cut up a fresh piece of gum, randomly select from it and an equivalent ‘dry’ piece of gum, and do 5 rounds of dual n-back to test attention/energy & WM. (If it turns out to be placebo, I’ll immediately use the remaining active dose: no sense in wasting gum, and this will test whether nigh-daily use renders nicotine gum useless, similar to how caffeine may be useless if taken daily. If there’s 3 pieces of active gum left, then I wrap it very tightly in Saran wrap which is sticky and air-tight.) The dose will be 1mg or 1/4 a gum. I cut up a dozen pieces into 4 pieces for 48 doses and set them out to dry. Per the previous power analyses, 48 groups of DNB rounds likely will be enough for detecting small-medium effects (partly since we will be only looking at one metric - average % right per 5 rounds - with no need for multiple correction). Analysis will be one-tailed, since we’re looking for whether there is a clear performance improvement and hence a reason to keep using nicotine gum (rather than whether nicotine gum might be harmful).
Cost-wise, the gum itself (~$5) is an irrelevant sunk cost and the DNB something I ought to be doing anyway. If the results are negative (which I’ll define as d < 0.2), I may well drop nicotine entirely since I have no reason to expect other forms (patches) or higher doses (2mg+) to create new benefits. This would save me an annual expense of ~$40 with a net present value of <820($); even if we count the time-value of the 20 minutes for the 5 DNB rounds over 48 days (0.2⋅48⋅7.25=70), it’s still a clear profit to run a convincing experiment.
First, we’ll check the prediction score (versus a random guesser scoring 0; higher is better):
logBinaryScore =sum.map (\(result,p) ->if result then1+logBase2 p else1+logBase2 (1-p))logBinaryScore [(True,0.35),(False,0.40),(False,0.40),(True,0.60),(True,0.35),(False,0.45),(False,0.50), (True,0.60),(False,0.30),(True,0.50),(False,0.40),(False,0.30),(False,0.25),(False,0.75), (False,0.40),(False,0.40),(False,0.65),(False,0.45),(True,0.50),(False,0.65),(True,0.40), (True,0.55),(True,0.40),(False,0.50),(False,0.60),(True,0.40),(False,0.50),(False,0.50), (False,0.55),(True,0.55),(False,0.50),(False,0.55),(False,0.45),(True,0.55),(True,0.50), (True,0.50),(False,0.55),(True,0.50)]-- -0.58
Ouch, so my guesses were actually worse than random; this isn’t encouraging (if nicotine was helpful, why didn’t I notice? Has 1mg tolerated?) but it does indicate the blinding was successful.
Now we will examine the actual performance. Extracting the individual rounds scores from my Brain Workshop log file, we can average them in groups of 5 to get a daily average; then feed them into BEST (Bayesian equivalent of t-test; see Kruschke 2012):
Daily data means, differences of inferred standard deviations & effect sizes: BESTplot(on2, off2, mcmcChain=mcmc, ROPEeff=c(0.1,1.5))
We can read off the results from the table or graph: the nicotine days average 1.1% higher, for an effect size of 0.24; however, the 95% credible interval (equivalent of confidence interval) goes all the way from 0.93 to -0.44, so we cannot exclude 0 effect and certainly not claim confidence the effect size must be >0.1. Specifically, the analysis gives a 66% chance that the effect size is >0.1. (One might wonder if any increase is due purely to a “training effect” - getting better at DNB. Probably not27.)
This is disappointing.
One curious thing that leaps out looking at the graphs is that the estimated underlying standard deviations differ: the nicotine days have a strikingly large standard deviation, indicating greater variability in scores - both higher and lower, since the means weren’t very different. The difference in standard deviations is just 6.6% below 0, so the difference almost reaches our usual frequentist levels of confidence too, which we can verify by testing:
var.test(on2, off2, alternative="greater")# F test to compare two variances## data: on2 and off2# F = 1.9823, num df = 15, denom df = 23, p-value = 0.06775# alternative hypothesis: true ratio of variances is greater than 1# 95% confidence interval:# 0.9314525 Inf# sample estimates:# ratio of variances# 1.982333
We can double-check this by seeing what the variance is for the unaveraged scores: we know the means are only 1.1% different, so the additional standard deviation must be coming from how individual days are good or bad, and if that is so, then unaveraging them out to eliminate most of the observed difference. We re-run BEST:
Means, differences of inferred standard deviations & effect sizes: BESTplot(on, off, mcmcChain=mcmc, ROPEeff=c(0.1,1.5))
We see the standard deviation difference go away - now the difference estimate is almost centered on zero with a just 75% estimate the standard deviation differs in the observed direction. And to repeat the frequentist test:
var.test(on, off, alternative="greater")# F test to compare two variances## data: on and off# F = 0.8564, num df = 79, denom df = 119, p-value = 0.7689# alternative hypothesis: true ratio of variances is greater than 1# 95% confidence interval:# 0.6140736 Inf# sample estimates:# ratio of variances# 0.856387
(So our p-value there went 0.06 → 0.769 when we disaggregated the days, consistent with the Bayesian results.)
The greatly increased variance, but only somewhat increased mean, is consistent with nicotine operating on me with an inverted U-curve for dosage/performance (or the Yerkes-Dodson law): on good days, 1mg nicotine is too much and degrades performance (perhaps I am overstimulated and find it hard to focus on something as boring as n-back) while on bad days, nicotine is just right and improves n-back performance.
This would be easy to test if I had done something before taking the nicotine gum; then I would simply see if pre-gum scores were higher than post-gum scores on nicotine days, but equal on placebo days. Unfortunately, I didn’t.
The closest data I have is my daily log of productivity/mood (1-5). If nicotine scores are higher than placebo scores on bad days (1-2) and lower on good days (3-4), then I think that would be consistent with an inverted U-curve.
nicotine <-read.table(stdin(),header=TRUE)day active mp score201208241335.2201208270537.2201208280337.6201208301337.75201208311237.75201209020236.0201209050536.0201209061537.25201209100549.2201209111336.8201209120344.6201209130538.4201209150543.8201209160239.6201209180349.6201209190438.4201209230536.2201209240545.4201209251343.8201209260436.4201209291343.8201209301336.0201210011346.0201210020445.0201210080234.6201210091345.2201210120537.8201210130437.2201210160440.2201210201339.0201210210341.2201210220342.2201210240540.4201210291241.4201210311338.4201211011543.8201211020348.2201211031540.6summary(nicotine)# day active mp score# Min. :20120824 Min. :0.0000 Min. :2.000 Min. :34.60# 1st Qu.:20120911 1st Qu.:0.0000 1st Qu.:3.000 1st Qu.:37.21# Median :20120926 Median :0.0000 Median :3.000 Median :39.30# Mean :20120954 Mean :0.3947 Mean :3.632 Mean :40.47# 3rd Qu.:20121015 3rd Qu.:1.0000 3rd Qu.:5.000 3rd Qu.:43.80# Max. :20121103 Max. :1.0000 Max. :5.000 Max. :49.60cor(nicotine)# day active mp score# day 0.05331968 0.07437166 0.32021554# active -0.27754064 -0.05727501# mp 0.05238032
Plot scores for each mood/productivity level, split between placebo & nicotine: boxplot(nicotine$score ~ (nicotine$active + nicotine$mp)^2)
Interesting. On days ranked ‘2’ (below-average mood/productivity), nicotine seems to have boosted scores; on days ranked ‘3’, nicotine hurts scores; there aren’t enough ‘4’s to tell, but even ’5’ days seem to see a boost from nicotine, which is not predicted by the theory. But I don’t think much of a conclusion can be drawn: not enough data to make out any simple relationship. Some modeling suggests no relationship in this data either (although also no difference in standard deviations, leading me to wonder if I screwed up the data recording - not all of the DNB scores seem to match the input data in the previous analysis). So although the ‘2’ days in the graph are striking, the theory may not be right.
The poor prediction performance, while confirming my belief that my novel strategy for blinding nicotine gum worked well, undermines confidence in the value of nicotine.
I specified at the beginning that I wanted an effect size of >0.2; I got it, but with it came a very wide credible interval, undermining confidence in the effect size.
The difference in standard deviations is not, from a theoretical perspective, all that strange a phenomenon: at the very beginning of this page, I covered some basic principles of nootropics and mentioned how many stimulants or supplements follow an inverted U-curve where too much or too little lead to poorer performance (ironically, one of the examples in Kruschke 201214ya was a smart drug which did not affect means but increased standard deviations).
If this is the case, this suggests some thoughtfulness about my use of nicotine: there are times when use of nicotine will not be helpful, but times where it will be helpful. I don’t know what makes the difference, but I can guess it relates to over-stimulation: on some nights during the experiment, I had difficult concentrating on n-backing because it was boring and I was thinking about the other things I was interested in or working on—in retrospect, I wonder if those instances were nicotine nights.
In retrospect, there were 2 parts of the experiment design I probably should have changed:
I used 1mg gum, rather than 2mg
1mg may have too small effects to easily detect, and I may have developed tolerance to 1mg even though I’ve been careful to space out all my gum use. 2mg would have reduced this concern.
I used 1mg each day regardless of the randomization
This was to make each day more consistent and avoid wasting a sliced piece of gum (due to evaporation, it’s use-it-or-lose-it). But this plausibly is a source of tolerance, and even #1 was not an issue when the self-experiment began, this could have become an issue.
All things considered, I will probably continue using nicotine gum sparingly.
Running low on gum (even using it weekly or less, it still runs out), I decided to try patches. Reading through various discussions, I couldn’t find any clear verdict on what patch brands might be safer (in terms of nicotine evaporation through a cut or edge) than others, so I went with the cheapest Habitrol I could find as a first try of patches (“Nicotine Transdermal System Patch, Stop Smoking Aid, 21 mg, Step 1, 14 patches”) in May 201313ya. I am curious to what extent nicotine might improve a long time period like several hours or a whole day, compared to the shorter-acting nicotine gum which feels like it helps for an hour at most and then tapers off (which is very useful in its own right for kicking me into starting something I have been procrastinating on). I have not decided whether to try another self-experiment.
Using the 21mg patches, I cut them into quarters. What I would do is I would cut out 1 quarter, and then seal the two edges with scotch tape, and put the Pac-Man back into its sleeve. Then the next time I would cut another quarter, seal the new edge, and so on. I thought that 5.25mg might be too much since I initially found 4mg gum to be too much, but it’s delivered over a long time and it wound up feeling much more like 1mg gum used regularly. I don’t know if the tape worked, but I did not notice any loss of potency. I didn’t like them as much as the gum because I would sometimes forget to take off a patch at the end of the day and it would interfere with sleep, and because the onset is much slower and I find I need stimulants more for getting started than for ongoing stimulation so it is better to have gum which can be taken precisely when needed and start acting quickly. (One case where the patches were definitely better than the gum was long car trips where slow onset is fine, since you’re most alert at the start.) When I finally ran out of patches in June 2016 (using them sparingly), I ordered gum instead.
Related to the famous -racetams but reportedly better (and much less bulky), Noopept is one of the many obscure Russian nootropics. (Further reading: Google Scholar, Examine.com, Reddit, Longecity, Bluelight.ru.) Its advantages seem to be that it’s far more compact than piracetam and doesn’t taste awful so it’s easier to store and consume; doesn’t have the cloud hanging over it that piracetam does due to the FDA letters, so it’s easy to purchase through normal channels; is cheap on a per-dose basis; and it has fans claiming it is better than piracetam.
A Redditor ordered some Russian brand Noopept, but finding it was unpleasant & not working for him, gave the left-over half to me:
Russian Noopept box, front & back
Russian Noopept blister-pack, front & back
It appeared in reasonably good shape, and closely matched the photographs in the Wikipedia article. I took 2 of the 25 10mg pills on successive days on top of my usual caffeine+piracetam stack, and didn’t notice anything; in particular, I didn’t find it unpleasant like he did.
So, I thought I might as well experiment since I have it. I put the 23 remaining pills into gel capsules with brown rice as filling, made ~30 placebo capsules, and will use the one-bag blinding/randomization method. I don’t want to spend the time it would take to n-back every day, so I will simply look for an effect on my daily mood/productivity self-rating; hopefully Noopept will add a little on average above and beyond my existing practices like caffeine+piracetam (yes, Noopept may be as good as piracetam, but since I still have a ton of piracetam from my 3kg order, I am primarily interested in whether Noopept adds onto piracetam rather than replaces). 10mg doses seem to be on the low side for Noopept users, weakening the effect, but on the other hand, if I were to take 2 capsules at a time, then I’d halve the sample size; it’s not clear what is the optimal tradeoff between dose and n for statistical power.
Nor am I sure how important the results are - partway through, I haven’t noticed anything bad, at least, from taking Noopept. And any effect is going to be subtle: people seem to think that 10mg is too small for an ingested rather than sublingual dose and I should be taking twice as much, and Noopept’s claimed to be a chronic gradual sort of thing, with less of an acute effect. If the effect size is positive, regardless of statistical-significance, I’ll probably think about doing a bigger real self-experiment (more days blocked into weeks or months & 20mg dose)
I don’t expect to find an effect, though; a quick t-test power analysis of a one-sided paired design with 23 pairs suggests that a reasonable power of 80% would still only be able to detect an increase of d>=0.5:
pwr.t.test(n=23, type="paired", alternative="greater", sig.level=0.05, power=0.8)# Paired t test power calculation## n = 23# d = 0.5352
Or in other words, since the standard deviation of my previous self-ratings is 0.75 (see the Weather and my productivity data), a mean rating increase of >0.39 on the self-rating. This is, unfortunately, implying an extreme shift in my self-assessments (for example, 3s are ~50% of the self-ratings and 4s ~25%; to cause an increase of 0.25 while leaving 2s alone in a sample of 23 days, one would have to push 3s down to ~25% and 4s up to ~47%). So in advance, we can see that the weak plausible effects for Noopept are not going to be detected here at our usual statistical levels with just the sample I have (a more plausible experiment might use 178 pairs over a year, detecting down to d>=0.18). But if the sign is right, it might make Noopept worthwhile to investigate further. And the hardest part of this was just making the pills, so it’s not a waste of effort.
Some quick tests turn in similar conclusions: both Noopept and the “Magtein” increased self-rating but not statistically-significantly (as expected from the beginning due to the lack of power).
npt <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2013-gwern-noopept.csv")wilcox.test(MP ~ Noopept, alternative="less", data = npt)## Wilcoxon rank sum test with continuity correction## data: MP by Noopept# W = 343, p-value = 0.2607summary(lm(MP ~ Noopept + Magtein, data = npt))# ...Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 2.8038 0.1556 18.02 <2e-16# Noopept 0.0886 0.2098 0.42 0.67# Magtein 0.2673 0.2070 1.29 0.20## Residual standard error: 0.761 on 53 degrees of freedom# Multiple R-squared: 0.0379, Adjusted R-squared: 0.00164# F-statistic: 1.05 on 2 and 53 DF, p-value: 0.359
More specifically, the ordinal logistic regression estimates effect sizes of odds-ratio 1.3 for the Noopept and 1.9 for the magnesium:
The magnesium was neither randomized nor blinded and included mostly as a covariate to avoid confounding (the Noopept coefficient & t-value increase somewhat without the Magtein variable), so an OR of 1.9 is likely too high; in any case, this experiment was too small to reliably detect any effect (~26% power, see bootstrap power simulation in the magnesium section) so we can’t say too much.
set.seed(3333)library(boot)noopeptPower <-function(dt, indices) { d <- dt[indices,] # bootstrap's _n_ = original _n_ lmodel <-lrm(MP ~ Noopept + Magtein, data = d)return(anova(lmodel)[7]) # _p_-value for the Noopept coefficient}bs <-boot(data=npt, statistic=noopeptPower, R=100000, parallel="multicore", ncpus=4)alpha <-0.05print(sum(bs$t<=alpha) /length(bs$t))# [1] 0.073
So for the observed effect size, the small Noopept sample had only 7% power to turn in a statistically-significant result. Given the plausible effect size, and weakness of the experiment, I find these results encouraging.
Noopept is a Russian stimulant sometimes suggested for nootropics use as it may be more effective than piracetam or other -racetams, and its smaller doses make it more convenient & possibly safer. Following up on a pilot study, I ran a well-powered blind randomized self-experiment between September 201313ya and August 201412ya using doses of 12-60mg Noopept & pairs of 3-day blocks to investigate the impact of Noopept on self-ratings of daily functioning in addition to my existing supplementation regimen involving small-to-moderate doses of piracetam. A linear regression, which included other concurrent experiments as covariates & used multiple imputation for missing data, indicates a small benefit to the lower dose levels and harm from the highest 60mg dose level, but no dose nor Noopept as a whole was statistically-significant. It seems Noopept’s effects are too subtle to easily notice if they exist, but if one uses it, one should probably avoid 60mg+.
In avoiding experimenting with more Russian Noopept pills and using instead the easily-purchased powder form of Noopept, there are two opposing considerations: Russian Noopept is reportedly the best, so we might expect anything I buy online to be weaker or impure or inferior somehow and the effect size smaller than in the pilot experiment; but by buying my own supply & using powder I can double or triple the dose to 20mg or 30mg (to compensate for the original under-dosing of 10mg) and so the effect size larger than in the pilot experiment.
As it happened, Health Supplement Wholesalers (since renamedPowder City) offered me a sample of their products, including their 5g Noopept powder ($13). I’d never used HSW before & they had some issues in the past; but I haven’t seen any recent complaints, so I was willing to try them. My 5g from batch #130830 arrived quickly (photos: packaging, powder contents). I tried some (tastes just slightly unpleasant, like an ultra-weak piracetam), and I set about capping the fluffy white flour-like powder with the hilariously tiny scoop they provide.
It took 4 hours to cap 432 Noopept pills and another 432 flour pills. I tried to allocate the Noopept as evenly as possible (3 little scoops per pill) which the HSW packaging suggested would be 10-30mg; running out after 432 implies I managed to get ~12mg into each (5000432=11.6). At 2 pills a day, the experiment will run under a year.
I don’t want to synchronize with the magnesium or lithium experiments, so I’ll use paired blocks of 3 days randomized 50:50, which will help with the reported tolerance of Noopept setting in after a few days and one needing to ‘cycle’.
To make things more interesting, I think I would like to try randomizing different dosages as well: 12mg, 24mg, and 36mg (1-3 pills); on 2014-05-05, because I wanted to finish up the experiment earlier, I decided to add 2 larger doses of 48 & 60mg (4-5 pills) as options. Then I can include the previous pilot study as 10mg doses, and regress over dose amount.
During this time period, I generally refrained from using any nicotine (I wound up using it only 3x in the experimental period) or modafinil (0x) to avoid adding variation to results. I did use magnesium citrate & LLLT (discussed later). Finally, I was taking a stack like this:
1mg melatonin at bedtime
5000IU vitamin D & multivitamin at morning; an iron supplement every 3 days
from 25 March to 2014-09-18, ~5g of creatine monohydrate per day
a few times a day, taking a custom gel pill which in total supplies ~1g piracetam & 200mg caffeine
I’ll first assume the effect size is the same. Using the usual alpha, we can find the necessary sample size by a slight variation on the magnesium bootstrap power calculation. Since the 56 days gave a power of 7% while we want closer to 80%, we probably want to start our power estimation much higher, with n in the 300s:
library(boot)library(rms)npt <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2013-gwern-noopept.csv")newNoopeptPower <-function(dt, indices) { d <- dt[sample(nrow(dt), n, replace=TRUE), ] # new dataset, possibly larger than the original lmodel <-lrm(MP ~ Noopept + Magtein, data = d)return(anova(lmodel)[7])}alpha <-0.05for (n inseq(from =300, to =600, by =30)) { bs <-boot(data=npt, statistic=newNoopeptPower, R=10000, parallel="multicore", ncpus=4)print(c(n, sum(bs$t<=alpha)/length(bs$t)))}# 0.18/0.19/0.21/0.21/0.23/0.25/0.26/0.28/0.29/0.32/0.32
Even at n = 600 (nearly 2 years), the estimated power is only 32%. This is absurdly small and such an experiment would be a waste of time.
Suppose we were optimistic and we doubled the effect 0.23 → 0.47 (this can be done by editing the first two Noopept rows and incrementing the MP variable by 1), and then looked again at power? At n = 300, power has reached 60%, and by n = 530, we have hit the desired 80%.
30mg: 10 - 11 March: 0; accidentally unblinded & restarted on the 12th (a spare rice placebo, which is visibly different from the flour/Noopept capsules, was mixed in)
Analyzing the results is a little tricky because I was simultaneously running the first magnesium citrate self-experiment, which turned out to cause a quite complex result which looks like a gradually-accumulating overdose negating an initial benefit for net harm, and also toying with LLLT, which turned out to have a strong correlation with benefits. So for the potential small Noopept effect to not be swamped, I need to include those in the analysis. I designed the experiment to try to find the best dose level, so I want to look at an average Noopept effect but also the estimated effect at each dose size in case some are negative (especially in the case of 5-pills/60mg); I included the pilot experiment data as 10mg doses since they were also blind & randomized. Finally, ‘missingness’ affects analysis: because not every variable is recorded for each date (what was the value of the variable for the blind randomized magnesium citrate before and after I finished that experiment? what value do you assign the Magtein variable before I bought it and after I used it all up?), just running a linear regression may not work exactly as one expects as various days get omitted because part of the data was missing.
noopeptSecond <-read.csv("https://gwern.net/doc/nootropic/quantified-self/2013-2014-gwern-noopept.csv", colClasses=c("Date","integer","integer","integer","logical"))l <-lm(MP ~ Noopept + LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date),data=noopeptSecond)summary(l)# Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 24.254373177 14.252905125 1.70171 0.09043607# Noopept 0.002069507 0.003937337 0.52561 0.59976836# LLLTTRUE 0.330112028 0.096133360 3.43390 0.00072963# as.logical(Magnesium.citrate)TRUE 27.058060337 19.655569654 1.37661 0.17024431# as.integer(Date) -0.001313316 0.000886616 -1.48127 0.14018300# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.001699162 0.001222719 -1.38966 0.16625033## Residual standard error: 0.640741 on 191 degrees of freedom# (731 observations deleted due to missingness)# Multiple R-squared: 0.154383, Adjusted R-squared: 0.132246# F-statistic: 6.97411 on 5 and 191 DF, p-value: 5.23897e-06
As expected since most of the data overlaps with the previous LLLT analysis, the LLLT variable correlates strongly; the individual magnesium variables may look a little more questionable but were justified in the magnesium citrate analysis. The Noopept result looks a little surprising - almost zero effect? Let’s split by dose (which was the point of the whole rigmarole of changing dose levels):
l2 <-lm(MP ~as.factor(Noopept) + LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date),data=noopeptSecond)summary(l2)# Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 27.044709119 14.677995235 1.84253 0.06697191# as.factor(Noopept)10 0.099920147 0.139287051 0.71737 0.47403711# as.factor(Noopept)15 0.526389063 0.297940313 1.76676 0.07889108# as.factor(Noopept)20 0.114943375 0.147994400 0.77667 0.43832733# as.factor(Noopept)30 0.019029776 0.125504996 0.15163 0.87964479# LLLTTRUE 0.329976497 0.096071943 3.43468 0.00072993# as.logical(Magnesium.citrate)TRUE 25.615810606 20.397271406 1.25584 0.21073068# as.integer(Date) -0.001488184 0.000913563 -1.62899 0.10499001# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.001610059 0.001269219 -1.26854 0.20617256## Residual standard error: 0.639823 on 188 degrees of freedom# (731 observations deleted due to missingness)# Multiple R-squared: 0.170047, Adjusted R-squared: 0.13473# F-statistic: 4.81487 on 8 and 188 DF, p-value: 2.08804e-05
This looks interesting: the Noopept effect is positive for all the dose levels, but it looks like a U-curve - low at 10mg, high at 15mg, lower at 20mg, and even lower at 30mg 48mg and 60mg aren’t estimated because they are hit by the missingness problem: the magnesium citrate variable is unavailable for the days the higher doses were taken on, and so their days are omitted and those levels of the factor are not estimated. One way to fix this is to drop magnesium from the model entirely, at the cost of fitting the data much more poorly and losing a lot of R2:
l3 <-lm(MP ~as.factor(Noopept) + LLLT, data=noopeptSecond)summary(l3)# Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 3.0564075 0.0578283 52.85318 < 2.22e-16# as.factor(Noopept)10 0.1079878 0.1255354 0.86022 0.39031118# as.factor(Noopept)15 0.1835389 0.2848069 0.64443 0.51975512# as.factor(Noopept)20 0.1314225 0.1301826 1.00952 0.31348347# as.factor(Noopept)30 0.0125616 0.1091561 0.11508 0.90845401# as.factor(Noopept)48 0.2302323 0.2050326 1.12291 0.26231647# as.factor(Noopept)60 -0.1714377 0.1794377 -0.95542 0.34008626# LLLTTRUE 0.2801608 0.0829625 3.37696 0.00082304## Residual standard error: 0.685953 on 321 degrees of freedom# (599 observations deleted due to missingness)# Multiple R-squared: 0.0468695, Adjusted R-squared: 0.0260848# F-statistic: 2.25499 on 7 and 321 DF, p-value: 0.0297924
This doesn’t fit the U-curve so well: while 60mg is substantially negative as one would extrapolate from 30mg being ~0, 48mg is actually better than 15mg. But we bought the estimates of 48mg/60mg at a steep price - we ignore the influence of magnesium which we know influences the data a great deal. And the higher doses were added towards the end, so may be influenced by the magnesium starting/stopping. Another fix for the missingness is to “impute” the missing data. In this case, we might argue that the placebo days of the magnesium experiment were identical to taking no magnesium at all and so we can classify each NA as a placebo day, and rerun the desired analysis:
The 48mg/60mg coefficients shift downwards as expected. If we plot the coefficients with arm’s coefplot(), and one squints, the confidence intervals/point-values for Noopept look sort of consistent with a U-curve. What if we switch to a quadratic term to try to turn the Noopept values into a curve?
li2 <-lm(MP ~ Noopept +I(Noopept^2) + LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date),data=noopeptImputed)summary(li2)# Coefficients:# Estimate Std. Error t value Pr(>|t|)# (Intercept) 9.172594278 8.112803113 1.13063 0.25905147# Noopept 0.008079500 0.006074315 1.33011 0.18442378# I(Noopept^2) -0.000178179 0.000122736 -1.45172 0.14755366# LLLTTRUE 0.284419402 0.080959896 3.51309 0.00050627# as.logical(Magnesium.citrate)TRUE 41.589054331 16.141539488 2.57652 0.01042501# as.integer(Date) -0.000373812 0.000502850 -0.74339 0.45778931# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.002604384 0.001003433 -2.59547 0.00987860## Residual standard error: 0.665408 on 322 degrees of freedom# (599 observations deleted due to missingness)# Multiple R-squared: 0.100316, Adjusted R-squared: 0.0835521# F-statistic: 5.98394 on 6 and 322 DF, p-value: 6.02357e-06
Looks better, but I’m not sure how well it fits. The quadratic y=0.0080795x+−0.000178179x2 has its maximum around 40mg, though, which seems suspiciously high; it seems that in order to fit the negative estimate for 60mg, the ‘top’ of the curve gets pulled over to 48mg since it’s almost as big as 15mg. I don’t find that entirely plausible.
A fancier method of imputation would be “multiple imputation” using, for example, the R library mice (“Multivariate Imputation by Chained Equations”) (guide), which will try to impute all missing values in a way which mimicks the internal structure of the data and provide several ‘possible’ datasets to give us an idea of what the underlying data might have looked like, so we can see how our estimates improve with no missingness & how much of the estimate is now due to the imputation:
library(mice)## work around apparent error in MICE: can't handle Dates type## even though no missing-values in that column...?noopeptSecond$Date <-as.integer(noopeptSecond$Date)nimp <-mice(noopeptSecond, m=200, maxit=200)li3 <-with(nimp, lm(MP ~ Noopept +I(Noopept^2) + LLLT +as.logical(Magnesium.citrate) +as.integer(Date) +as.logical(Magnesium.citrate):as.integer(Date)))round(summary(pool(li3)), 4)# est se t df Pr(>|t|)# (Intercept) -8.3369 3.2520 -2.5636 296.1619 0.0109# Noopept 0.0073 0.0057 1.2790 521.5756 0.2015# I(Noopept^2) -0.0001 0.0001 -1.2808 583.2136 0.2008# LLLT 0.3069 0.0910 3.3737 168.4541 0.0009# as.logical(Magnesium.citrate)TRUE 7.0763 3.9584 1.7877 298.7476 0.0748# as.integer(Date) 0.0007 0.0002 3.4911 299.6728 0.0006# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.0005 0.0002 -1.8119 300.7040 0.0710# lo 95 hi 95 nmis fmi lambda# (Intercept) -14.7369 -1.9368 NA 0.4974 0.4940# Noopept -0.0039 0.0185 457 0.2852 0.2824# I(Noopept^2) -0.0004 0.0001 NA 0.2411 0.2385# LLLT 0.1273 0.4864 599 0.6954 0.6918# as.logical(Magnesium.citrate)TRUE -0.7135 14.8662 NA 0.4942 0.4908# as.integer(Date) 0.0003 0.0011 NA 0.4930 0.4897# as.logical(Magnesium.citrate)TRUE:as.integer(Date) -0.0009 0.0000 NA 0.4918 0.4884
The coefficients & p-values agree, so it seems that it doesn’t make too much difference how we deal with missingness.
Finally, we can see if some weak priors/regularization changes the picture much by using a Bayesian regression instead:
The 95% credible intervals emphasize that while the mean estimates of the posterior for the Noopept parameters are positive, there’s substantial uncertainty after updating on the data, and the effects are small.
Should I run another followup experiment? No; the implied effect is so small a confirmatory experiment would have to run a miserably long time, it seems:
So on net, I think there may be an effect but it’s small and I don’t know whether the optimal dose would be lower (~10mg) or much higher (~40mg). I don’t find this a particularly good reason to continue taking Noopept: it seems to either not be helpful in a noticeable way or to be redundant with the piracetam.
Oxiracetam is one of the 3 most popular -racetams; less popular than piracetam but seems to be more popular than aniracetam. Prices have come down substantially since the early 2000s, and stand at around 1.2g/$ or roughly 50 cents a dose, which was low enough to experiment with; key question, does it stack with piracetam or is it redundant for me? (Oxiracetam can’t compete on price with my piracetam pile stockpile: the latter is now a sunk cost and hence free.)
I bought 60 grams from Smart Powders and combined it with the DMAE; I couldn’t compare oxiracetam+DMAE vs oxiracetam+choline-bitartrate because I had capped all the choline with the piracetam. One immediate advantage of oxiracetam: it is not unbelievably foul tasting like piracetam, but slightly sweet.
Regardless, while in the absence of piracetam, I did notice some stimulant effects (somewhat negative - more aggressive than usual while driving) and similar effects to piracetam, I did not notice any mental performance beyond piracetam when using them both. The most I can say is that on some nights, I seemed to be less easily tired when writing or editing or n-backing, but those were also often nights I was also trying out all the other things I had gotten in that order from Smart Powders, and I am still dis-entangling what was responsible. (Probably the l-theanine or sulbutiamine.)
In other words, for me, the two -racetams did not seem to ‘stack’. The following are a number of n-back scores from before (piracetam only) and after (piracetam and oxiracetam):
There may be some improvement hidden in there, but nothing jumps out to my eye. Oxiracetam has smaller recommended doses than piracetam, true, but even after taking that into account, oxiracetam is still more expensive per dose. When I finished it off, I decided it hadn’t shown any benefits so there was no point in continuing it.
I bought 500g of piracetam (Examine.com; FDA adverse events) from Smart Powders (piracetam is one of the cheapest nootropics and SP was one of the cheapest suppliers; the others were much more expensive as of October 201016ya), and I’ve tried it out for several days (started on 2009-09-07, and used it steadily up to mid-December). I’ve varied my dose from 3 grams to 12 grams (at least, I think the little scoop measures in grams), taking them in my tea or bitter fruit juice. Cranberry worked the best, although orange juice masks the taste pretty well; I also accidentally learned that piracetam stings horribly when I got some on a cat scratch. 3 grams (alone) didn’t seem to do much of anything while 12 grams gave me a nasty headache. I also ate 2 or 3 eggs a day.
Subjectively, I didn’t notice drastic changes. Here’s what I did notice:
My thinking seems a little clearer
I’m not so easy to tire - I went through a month’s worth of my Wikipedia watchlist with less fatigue than usual, and n-backing doesn’t seem so tiring.
DNB-wise, eyeballing my stats file seems to indicate a small increase: when I compare peak scores D4B scores, I see mostly 50s and a few 60s before piracetam, and after starting piracetam, a few 70s mixed into the 50s and 60s. Natural increase from training? Dunno - I’ve been stuck on D4B since June, so 5 or 10% in a week or 3 seems a little suspicious. A graph of the score series28:
The other day, I also noticed I was fidgeting less
After a week or two, I think I noticed better reflexes - both in catching falling cups and the saccading in BW seems slightly easier. But I could be imagining this since I just saw an Erowid report mentioning better reflexes & I may’ve read that one before I started. (Darn those subconscious impressions and memories! :)
After 7 days, I ordered a kg of choline bitartrate from Bulk Powders. Choline is standard among piracetam-users because it is pretty universally supported by anecdotes about “piracetam headaches”, has support in rat/mice experiments29, and also some human-related research. So I figured I couldn’t fairly test piracetam without some regular choline - the eggs might not be enough, might be the wrong kind, etc. It has a quite distinctly fishy smell, but the actual taste is more citrus-y, and it seems to neutralize the piracetam taste in tea (which makes things much easier for me).
The first day (22 September) I took ~10g since I was taking 5g of piracetam; I wound up with some diarrhea & farting. Oops.
On the plus side: - I noticed the less-fatigue thing to a greater extent, getting out of my classes much less tired than usual. (Caveat: my sleep schedule recently changed for the saner, so it’s possible that’s responsible. I think it’s more the piracetam+choline, though.) - One thing I wasn’t expecting was a decrease in my appetite - nobody had mentioned that in their reports.I don’t like being bothered by my appetite (I know how to eat fine without it reminding me), so I count this as a plus. - Fidgeting was reduced further
The second day I went with ~6g of choline; much less intestinal distress, but similar effects vis-a-vis fidgeting, loss of appetite, & reduced fatigue. So in general I thought this was a positive experience, but I’m not sure it was worth $40 for ~2 months’ worth, and it was tedious consuming it dissolved.
Fortunately for me, the FDA decided Smart Powder’s advertising was too explicit and ordered its piracetam sales stopped; I was equivocal at the previous price point, but then I saw that between the bulk discount and the fire-sale coupon, 3kg was only $99.99 (shipping was amortized over that, the choline, caffeine, and tryptophan). So I ordered in September 2010. As well, I had decided to cap my own pills, eliminating the inconvenience and bad taste. 3kg goes a very long way so I am nowhere close to running out of my pills; there is nothing to report since, as the pills are simply part of my daily routine.
I take my piracetam in the form of capped pills consisting (in descending order) of piracetam, choline bitartrate, anhydrous caffeine, and l-tyrosine. On 2012-12-08, I happened to run out of them and couldn’t fetch more from my stock until 27 December. This forms a sort of (non-randomized, non-blind) short “natural experiment”: did my daily 1-5 mood/productivity ratings fall during 8-27 December compared to November 201214ya & January 201313ya? The graphed data30 suggests to me a decline:
See footnote for R code
The BEST results31 give a small effect size of -0.26 and only partial exclusion of zero effect size (which a one-tailed two-sample test agrees with32):
So the answer is yes, M/P did fall as I expected; but also as one would expect given daily variation and the small sample of ‘off’ days (19 days), the result is not very statistically robust (even ignoring the low quality of data from a natural experiment). But it was an easy ‘experiment’ to run and the result had the right sign, as they say.
In the 2011–201214yaQuantified Health Prize, potassium (FDA adverse events) came up twice as a recommendation. Potassium is vital to nerve conduction, since nerve impulses are nothing but potassium and sodium rushing around, but it didn’t seem like a priority to investigate since I am not an athlete nor do I sweat a great deal.
By which I mean that simple potassium is probably the most positively mind altering supplement I’ve ever tried…About 15 minutes after consumption, it manifests as a kind of pressure in the head or temples or eyes, a clearing up of brain fog, increased focus, and the kind of energy that is not jittery but the kind that makes you feel like exercising would be the reasonable and prudent thing to do. I have done no tests, but “feel” smarter from this in a way that seems much stronger than piracetam or any of the conventional weak nootropics. It is not just me – I have been introducing this around my inner social circle and I’m at 7/10 people felt immediately noticeable effects. The 3 that didn’t notice much were vegetarians and less likely to have been deficient. Now that I’m not deficient, it is of course not noticeable as mind altering, but still serves to be energizing, particularly for sustained mental energy as the night goes on…Potassium chloride initially, but since bought some potassium gluconate pills… research indicates you don’t want to consume large amounts of chloride (just moderate amounts).
…The first time I took supplemental potassium (50% US RDA in a lot of water), it was like a brain fog lifted that I never knew I had, and I felt profoundly energized in a way that made me feel exercise was reasonable and prudent, which resulted in me and the roommate that had just supplemented potassium going for an hour long walk at 2AM. Experiences since then have not been quite so profound (which probably was so stark for me as I was likely fixing an acute deficiency), but I can still count on a moderately large amount of potassium to give me a solid, nearly side effect free performance boost for a few hours…I had been doing Bikram yoga on and off, and I think I wasn’t keeping up the practice because I wasn’t able to properly rehydrate myself.
One claim was partially verified in passing by EliezerYudkowsky (“Supplementing potassium (citrate) hasn’t helped me much, but works dramatically for Anna, Kevin, and Vassar…About the same as drinking a cup of coffee - ie. it works as a perker-upper, somehow. I’m not sure, since it doesn’t do anything for me except possibly mitigate foot cramps.”)
I largely ignored this since the discussions were of sub-RDA doses, and my experience has usually been that RDAs are a poor benchmark and frequently far too low (consider the RDA for vitamin D). This time, I checked the actual RDA - and was immediately shocked and sure I was looking at a bad reference: there was no way the RDA for potassium was seriously 3700-4700mg or 4-5 grams daily, was there? Just as an American, that implied that I was getting less than half my RDA. (How would I get 4g of potassium in the first place? Eat a dozen bananas a day⸮) I am not a vegetarian, nor is my diet that fantastic: I figured I was getting some potassium from the ~2 fresh tomatoes I was eating daily, but otherwise my diet was not rich in potassium sources. I have no blood tests demonstrating deficiency, but given the figures, I cannot see how I could not be deficient.
Potassium is not the safest supplement ever, but it’s reasonably safe (kidneys can filter out overdoses), and between the anecdotes and my sudden realization that I was highly likely deficient, I decided to try it out.
Potassium citrate powder is neither expensive nor cheap: I purchased 453g for $21. The powder is crystalline white, dissolves instantly in water, and largely tasteless (sort of saline & slightly unpleasant). The powder is 37% potassium by weight (the formula is C6H5K3O7) so 453g is actually 167g of potassium, so 80-160 days’ worth depending on dose.
My first impression of ~1g around 12:30PM was that while I do not feel like running around, within an hour I did feel like the ‘brain fog’ was lighter than before. The effect wasn’t dramatic, so I can’t be very confident. Operationalizing ‘brain fog’ for an experiment might be hard: it doesn’t necessarily feel like I would do better on dual n-back. I took 2 smaller doses 3 and 6 hours later, to no further effect. Over the following weeks and months, I continued to randomly alternate between potassium & non-potassium days. I noticed no effects other than sleep problems.
That first night, I had severe trouble sleeping, falling asleep in 30 minutes rather than my usual 19.6±11.9, waking up 12 times (5.9±3.4), and spending ~90 minutes awake (18.1±16.2), and naturally I felt unrested the next day; I initially assumed it was because I had left a fan on (moving air keeps me awake) but the new potassium is also a possible culprit. When I asked, Kevin said:
I think a general high water high electrolyte diet has benefited my sleep. I haven’t noticed potassium immediately before bed decreasing sleep quality.
I began recording a subset of sleep data by hand as another sleep experiment. The conclusion was that there was a very strong negative effect on my sleep (d=-1.1) and no benefit to my mood/productivity self-ratings.
Since my experiment had a number of flaws (non-blind, varying doses at varying times of day), I wound up doing a second better experiment using blind standardized smaller doses in the morning. The negative effect was much smaller, but there was still no mood/productivity benefit. Having used up my first batch of potassium citrate in these 2 experiments, I will not be ordering again since it clearly doesn’t work for me.
Dosage is apparently 5-10mg a day. (Prices can be better elsewhere; selegiline is popular for treating dogs with senile dementia, where those 60x5mg will cost $2 rather than $3533. One needs a veterinarian’s prescription to purchase from pet-oriented online pharmacies, though.) I ordered it & modafinil from Nubrain.com at $35 for 60x5mg; Nubrain delayed and eventually canceled my order - and my enthusiasm. Between that and realizing how much of a premium I was paying for Nubrain’s deprenyl, I’m tabling deprenyl along with nicotine & modafinil for now. Which is too bad, because I had even ordered 20g of PEA from Smart Powders to try out with the deprenyl. (My later attempt to order some off the Silk Road also failed when the seller canceled the order.)
My general impression is positive; it does seem to help with endurance and extended the effect of piracetam+choline, but is not as effective as that combo. At $20 for 30g (bought from Smart Powders), I’m not sure it’s worthwhile, but I think at $10-15 it would probably be worthwhile. Sulbutiamine seems to affect my sleep negatively, like caffeine. I bought 2 or 3 canisters for my third batch of pills along with the theanine. For a few nights in a row, I slept terribly and stayed awake thinking until the wee hours of the morning; eventually I realized it was because I was taking the theanine pills along with the sleep-mix pills, and the only ingredient that was a stimulant in the batch was - sulbutiamine. I cut out the theanine pills at night, and my sleep went back to normal. (While very annoying, this, like the creatine & taekwondo example, does tend to prove to me that sulbutiamine was doing something and it is not pure placebo effect.)
It’s worth noting that sulbutiamine reports vary dramatically, and it seems possible that some people are thiamine-deficient and so would disproportionately; SilasBarta noticed little to nothing (like me), but Jimrandomh reports his life was transformed (and he suspects that his diabetes caused or exacerbated a deficiency).
Taurine (Examine.com) was another gamble on my part, based mostly on its inclusion in energy drinks. I didn’t do as much research as I should have: it came as a shock to me when I read in Wikipedia that “taurine has been shown to prevent oxidative stress induced by exercise” and was an antioxidant - oxidative stress is a key part of how exercise creates health benefits and antioxidants inhibit those benefits.
So now I have to be careful about when I take it so it isn’t near a session of exercise or just accept whatever damage taurine does me. I’m not sure what I’ll do with it when I cap my current supply of powders. (It would make little sense to cap it with the creatine since I would often take the creatine before exercise.)
And the effects? Well, if you look through the WP article or other places, you see it justified in part due to supposed long term benefits or effects on blood sugar. I can’t say I’ve noticed any absence of ‘crashes’, taking it on alternate days or alone. (At least it wasn’t too expensive - $9 for 500g.)
The hormone testosterone (Examine.com; FDA adverse events) needs no introduction. This is one of the scariest substances I have considered using: it affects so many bodily systems in so many ways that it seems almost impossible to come up with a net summary, either positive or negative. With testosterone, the problem is not the usual nootropics problem that that there is a lack of human research, the problem is that the summary constitutes a textbook - or two. That said, the 201115ya review “The role of testosterone in social interaction” (excerpts) gives me the impression that testosterone does indeed play into risk-taking, motivation, and social status-seeking; some useful links and a representative anecdote:
While the primary effect of the drug is massive muscle growth the psychological side effects actually improved his sanity by an absurd degree. He went from barely functional to highly productive. When one observes that the decision to not attempt to fulfill one’s CEV at a given moment is a bad decision it follows that all else being equal improved motivation is improved sanity.
Elaborating on why the psychological side effects of testosterone injection are individual dependent: Not everyone get the same amount of motivation and increased goal seeking from the steroid and most people do not experience periods of chronic avolition. Another psychological effect is a potentially drastic increase in aggression which in turn can have negative social consequences. In the case of counterfactual Wedrifid he gets a net improvement in social consequences. He has observed that aggression and anger are a prompt for increased ruthless self-interested goal seeking. Ruthless self-interested goal seeking involves actually bothering to pay attention to social politics. People like people who do social politics well. Most particularly it prevents acting on contempt which is what Wedrifid finds prompts the most hostility and resentment in others. Point is, what is a sanity promoting change in one person may not be in another.
As it happens, these are areas I am distinctly lacking in. When I first began reading about testosterone I had no particular reason to think it might be an issue for me, but it increasingly sounded plausible, an aunt independently suggested I might be deficient, a biological uncle turned out to be severely deficient with levels around 90 ng/dl (where the normal range for 20-49yo males is 249-839), and finally my blood test in August 201313ya revealed that my actual level was 305 ng/dl; inasmuch as I was 25 and not 49, this is a tad low.
One idea I’ve been musing about is the connections between IQ, Conscientiousness, and testosterone. IQ and Conscientiousness do not correlate to a remarkable degree - even though one would expect IQ to at least somewhat enable a long-term perspective, self-discipline, metacognition, etc.! There are indications in studies of gifted youth that they have lower testosterone levels. The studies I’ve read on testosterone indicate no improvements to raw ability. So, could there be a self-sabotaging aspect to human intelligence whereby greater intelligence depends on lack of testosterone, but this same lack also holds back Conscientiousness (despite one’s expectation that intelligence would produce greater self-discipline and planning), undermining the utility of greater intelligence? Could cases of high IQ types who suddenly stop slacking and accomplish great things sometimes be due to changes in testosterone? Studies on the correlations between IQ, testosterone, Conscientiousness, and various measures of accomplishment are confusing and don’t always support this theory, but it’s an idea to keep in mind.
One might suggest just going to the gym or doing other activities which may increase endogenous testosterone secretion. This would be unsatisfying to me as it introduces confounds: the exercise may be doing all the work in any observed effect, and certainly can’t be blinded. And blinding is especially important because the 201115ya review discusses how some studies report that the famed influence of testosterone on aggression (eg. Wedrifid’s anecdote above) is a placebo effect caused by the “folk wisdom” that testosterone causes aggression & rage!
I have a needle phobia, so injections are right out; but from the images I have found, it looks like testosterone enanthate gels using DMSO resemble other gels like Vaseline. This suggests an easy experimental procedure: spoon an appropriate dose of testosterone gel into one opaque jar, spoon some Vaseline gel into another, and pick one randomly to apply while not looking. If one gel evaporates but the other doesn’t, or they have some other difference in behavior, the procedure can be expanded to something like “and then half an hour later, take a shower to remove all visible traces of the gel”. Testosterone itself has a fairly short half-life of 2-4 hours, but the gel or effects might linger. (Injections apparently operate on a time-scale of weeks; I’m not clear on whether this is because the oil takes that long to be absorbed by surrounding materials or something else.) Experimental design will depend on the specifics of the obtained substance. As a controlled substance (Schedule III in the US), supplies will be hard to obtain; I may have to resort to the Silk Road.
Power-wise, the effects of testosterone are generally reported to be strong and unmistakable. Even a short experiment should work. I would want to measure DNB scores & Mnemosyne review averages as usual, to verify no gross mental deficits; the important measures would be physical activity, so either pedometer or miles on treadmill, and general productivity/mood. The former 2 variables should remain the same or increase, and the latter 2 should increase.
Either prescription or illegal, daily use of testosterone would not be cheap. On the other hand, if I am one of the people for whom testosterone works very well, it would be even more valuable than modafinil, in which case it is well worth even arduous experimenting. Since I am on the fence on whether it would help, this suggests the value of information is high.
l-theanine (Examine.com) is occasionally mentioned on Reddit or Imminst or LessWrong34 but is rarely a top-level post or article; this is probably because theanine was discovered a very long time ago (>61 years ago), and it’s a pretty straightforward substance. It’s a weak relaxant/anxiolytic (Google Scholar) which is possibly responsible for a few of the health benefits of tea, and whichworkssynergistically with caffeine (and is probably why caffeine delivered through coffee feels different from the same amount consumed in tea - in one study, separate caffeine and theanine were a mixed bag, but the combination beat placebo on all measurements). The half-life in humans seems to be pretty short, with van der Pijl 2010 putting it ~60 minutes. This suggests to me that regular tea consumption over a day is best, or at least that one should lower caffeine use - combining caffeine and theanine into a single-dose pill has the problem of caffeine’s half-life being much longer so the caffeine will be acting after the theanine has been largely eliminated. The problem with getting it via tea is that teas can vary widely in their theanine levels and the variations don’t seem to be consistent either, nor is it clear how to estimate them. (If you take a large dose in theanine like 400mg in water, you can taste the sweetness, but it’s subtle enough I doubt anyone can actually distinguish the theanine levels of tea; incidentally, r-theanine - the useless racemic other version - anecdotally tastes weaker and less sweet than l-theanine.)
On 2011-04-08, I purchased from Smart Powders (20g for $8); as before, some light searching seemed to turn up SP as the best seller given shipping overhead; it was on sale and I planned to cap it so I got 80g. This may seem like a lot, but I was highly confident that theanine and I would get along since I already drink so much tea and was a tad annoyed at the edge I got with straight caffeine. So far I’m pretty happy with it. My goal was to eliminate the physical & mental “twitchiness” of caffeine, which subjectively it seems to do.
Running low on my theanine in May 201313ya, I learned SP was now undercut by LiftMode selling 50g for $14, so I got 2 (I was doing a big Amazon order anyway). Like the SP theanine it is a nice fluffy white powder and seems to work as well.
A new all-in-one nootropic mix/company run by some people active on /r/nootropics; they offered me a month’s supply for free to try & review for them. At ~$150.11$1002013 a month (it depends on how many months one buys), it is not cheap (John Backus estimates one could buy the raw ingredients for $37.53$252013/month) but it provides convenience & is aimed at people uninterested in spending a great deal of time reviewing research papers & anecdotes or capping their own pills (ie. people with lives) and it’s unlikely I could spare the money to subscribe if TruBrain worked well for me - but certainly there was no harm in trying it out.
The ingredients list was sane and similar to what I would have chosen, and doesn’t include any jokers like caffeine:
Piracetam: 3g
Naturally, as piracetam is the standard -racetam to use. It’s always worked well for me. 3g is a reasonable amount for people who aren’t taking any other sources of piracetam.
ALCAR: 0.5g
I didn’t notice any personal benefits from ALCAR, but I didn’t notice any bad effects either and many people claim to benefit.
CDP-Choline: 0.25g
You’ll want choline when using -racetams. 0.25g strikes me as low.
EPA/DHA: 1.2g
Fish oil is a safe bet for supplements. 1.2g is also low, I would prefer double that. (In the batch I got, there was a sort of fruity/gummy taste & aftertaste. Apparently it’s cherry-flavored.)
Magnesium glycinate/lycinate: 0.2g
My magnesium l-threonate correlation from the Noopept self-experiment suggested magnesium would help me, so I don’t mind seeing magnesium here as well.
Like ALCAR, did nothing subjectively noticeable for me, but nothing bad either.
The packaging is nice, if a little confusing (it’s not entirely clear what packets are supposed to be taken on the initial days as part of the “loading”). The pills are swallowable (one takes a set with breakfast and a second set with lunch). I do not seem to have died or gone into untoward states like seizures, and the first day went swimmingly.
l-Tryptophan is in a sense redundant with taking melatonin, since melatonin is one of the most prominent metabolites of tryptophan. Nevertheless, subjectively I seem to sleep better by taking 1.5mg of melatonin & 0.5g of tryptophan than I do by taking, say, 3mg of melatonin.
One of the other suggested benefits is for boosting serotonin levels; low levels of serotonin are implicated in a number of issues like depression. I’m not yet sure whether tryptophan has helped with motivation or happiness. Trial and error has taught me that it’s a bad idea to take tryptophan in the morning or afternoon, however, even smaller quantities like 0.25g. Like melatonin, the dose-response curve is a U: ~1g is great and induces multiple vivid dreams for me, but ~1.5g leads to an awful night and a headache the next day that was worse, if anything, than melatonin. (One morning I woke up with traces of at least 7 dreams, although I managed to write down only 2. No lucid dreams, though.)
Taking the tryptophan is fairly difficult. The powder as supplied by Bulk Nutrition is extraordinarily dry and fine; it seems to be positively hydrophobic. The first time I tried to swallow a teaspoon, I nearly coughed it out - the power had seemed to explode in my mouth and go down my lungs. Thenceforth I made sure to have a mouth of water first. After a while, I took a different tack: I mixed in as much Hericium as would fit in the container. The mushroom powder is wetter and chunkier than the tryptophan, and seems to reduce the problem. Combining the mix with chunks of melatonin inside a pill works even better.
Tyrosine (Examine.com) is an amino acid; people on the Imminst.org forums (as well as Wikipedia) suggest that it helps with energy and coping with stress. I ordered 4oz (bought from Smart Powders) to try it out, and I began taking 1g with my usual caffeine+piracetam+choline mix. It does not dissolve easily in hot water, and is very chalky and not especially tasty. I have not noticed any particular effects from it.
There are a number of treatments for the last. I already use melatonin. I sort of have light therapy from a full-spectrum fluorescent desk lamp. But I get very little sunlight; the surprising thing would be if I didn’t have a vitamin D deficiency. And vitamin D deficiencies have been linked with all sorts of interesting things like near-sightedness, with time outdoors inversely correlating with myopia and not reading or near-work time. (It has been claimed that caffeine interferes with vitamin D absorption and so people like me especially need to take vitamin D, on top of the deficits caused by our vampiric habits, but I don’t think this is true36.) Unfortunately, there’s not very good evidence that vitamin D supplementation helps with mood/SAD/depression: there’s ~6 small RCTs with some findings of benefits, with their respective meta-analysis turning in a positive but currently non-statistically-significant result. Better confirmed is reducing all-cause mortality in elderly people (see, in order of increasing comprehensiveness: Evidence Syntheses 2013, Chung et al 2009, Autier & Gandini 2007, Bolland et al 2014).
Given the involvement with circadian rhythms and the synthesis involving direct sunlight, it is likely a bad idea to take vitamin D close to bedtime, and there have been anecdotes that it damages sleep quality; I investigated this with my Zeo and concluded it seemed to be true for me.
The soft gels are very small; one needs to be a bit careful - Vitamin D is fat-soluble and overdose starts in the range of 70,000 IU37, so it would take at least 14 pills, and it’s unclear where problems start with chronic use. Vitamin D, like many supplements, followsaU-shapedresponsecurve (see also Melamed et al 2008 and Durup et al 2012) - too much can be quite as bad as too little. Too little, though, is likely very bad. The previously cited studies with high acute doses worked out to <1,000 IU a day, so they may reassure us about the risks of a large acute dose but not tell us much about smaller chronic doses; the mortality increases due to too-high blood levels begin at ~140nmol/l and reading anecdotes online suggest that 5k IU daily doses tend to put people well below that (around 70-100nmol/l). I probably should get a blood test to be sure, but I have something of a needle phobia.
I have elsewhere remarked on the apparent lack of benefit to taking multivitamins and the possible harm; so one might well wonder about a specific vitamin like vitamin D. However, a ‘multivitamin’ is not ‘vitamin D’, so it’s no surprise that they might do different things. If a multivitamin had no vitamin D in it, or if it had vitamin D in different doses, or if it had substances which interacted with vitamin D (such as calcium), or if it had substances which had negative effects which outweigh the positive (such as vitamin A?), we could well expect differing results. In this case, all of those are true to varying extents. Some multivitamins I’ve had contained no vitamin D. The last multivitamin I was taking both contains vitamins used in the negative trials and also some calcium; the listed vitamin D dosage was a trivial ~400IU, while I take >10x as much now (5000IU).
10,000 IU is highly likely to be enough, and is similar to what one might get from an hour on the beach; so 5000 IU should be satisfactory.
With the more subtle nootropics, poor shopping can lead to the price per dose becoming so high that they are not cost-effective; this does not have to be the case.
This tendency is exacerbated by general inefficiencies in the nootropics market - they are manufactured for vastly less than they sell for, although the margins aren’t as high as they are in other supplement markets, and not nearly ascomical as illegal recreational drugs. (Global Price Fixing: Our Customers are the Enemy (Connor 200125ya) briefly covers the vitamin cartel that operated for most of the 20th century, forcing food-grade vitamins prices up to well over 100x the manufacturing cost.) For example, the notorious Timothy Ferriss (of The Four-hour Work Week) advises imitators to find a niche market with very high margins which they can insert themselves into as middlemen and reap the profits; one of his first businesses specialized in… nootropics & bodybuilding. Or, when Smart Powders - usually one of the cheapest suppliers - was dumping its piracetam in a fire sale of half-off after the FDA warning, its owner mentioned on forums that the piracetam was still profitable (and that he didn’t really care because selling to bodybuilders was so lucrative); this was because while SP was selling 2kg of piracetam for ~$90, Chinese suppliers were offering piracetam on AliBaba for $30 a kilogram or a third of that in bulk. (Of course, you need to order in quantities like 30kg - this is more or less the only problem the middlemen retailers solve.) It goes without saying that premixed pills or products are even more expensive than the powders.
Powders are good for experimenting with (easy to vary doses and mix), but not so good for regular taking. I use OO gel capsules with a Capsule Machine: it’s hard to beat $20, it works, it’s not that messy after practice, and it’s not too bad to do 100 pills. However, I once did 3kg of piracetam + my other powders, and doing that nearly burned me out on ever using capsules again. If you’re going to do that much, something more automated is a serious question! (What actually wound up infuriating me the most was when capsules would stick in either the bottom or top tray—requiring you to very gingerly pull and twist them out, lest the two halves slip and spill powder—or when the two halves wouldn’t lock and you had to join them by hand. In contrast: loading the gel caps could be done automatically without looking, after some experience.)
Manually mixing powders is too annoying, and pre-mixed pills are expensive in bulk. So if I’m not actively experimenting with something, and not yet rich, the best thing is to make my own pills, and if I’m making my own pills, I might as well make a custom formulation using the ones I’ve found personally effective. And since making pills is tedious, I want to not have to do it again for years. 3 years seems like a good interval - 1095 days. Since one is often busy and mayn’t take that day’s pills (there are enough ingredients it has to be multiple pills), it’s safe to round it down to a nice even 1,000 days. What sort of hypothetical stack could I make? What do the prices come out to be, and what might we omit in the interests of protecting our pocketbook?
We omit tryptophan and melatonin, of course, because they are most useful for sleeping and this is a stimulus pill for daytime usage. That leaves from the above the following, with some basic commercial specs from the usual retailers:
We calculate how many days each unit gets us simply by dose divided by dose per day. We get quite a range; with some products, we only need 4 units to cover at least 1,000 days, but we need 100 units for modafinil!
Ingredient
Units
Cost
aniracetam
6
$300
caffeine
5
$90
choline citrate
4
$68
creatine
4
$68
lithium orotate
8
$88
modafinil
100
$800
sulbutiamine
9
$180
theanine
5
$50
Sum total, $1,644, or $1.65 per day for the ingredients.
But how many pills does this make and how much do those pills cost?
Capsule Connection sells 1,000 00 pills (the largest pills) for $9. I already have a pill machine, so that doesn’t count (a sunk cost). If we sum the grams per day column from the first table, we get 9.75 grams a day. Each 00 pill can take around 0.75 grams, so we need 13 pills. (Creatine is very bulky, alas.) 13 pills per day for 1,000 days is 13,000 pills, and 1,000 pills is $9 so we need 13 units and 13 times 9 is $117.
Redoing the above, the total expense is $1,761 or $,1.76 per day.
13 pills a day sounds like a lot, and $1.76 is actually a fair amount per day compared to what most people take. If I couldn’t swing a round $1,800 (even to cover years of consumption), how would I economize?
Looking at the prices, the overwhelming expense is for modafinil. It’s a powerful stimulant - possibly the single most effective ingredient in the list - but dang expensive. Worse, there’s anecdotal evidence that one can develop tolerance to modafinil, so we might be wasting a great deal of money on it. (And for me, modafinil isn’t even very useful in the daytime: I can’t even notice it.) If we drop it, the cost drops by a full $800 from $1,761 to $,961 (almost halving) and to $0.96 per day. A remarkable difference, and if one were genetically insensitive to modafinil, one would definitely want to remove it.
On the other metric, suppose we removed the creatine? Dropping 4 grams of material means we only need to consume 5.75 grams a day, covered by 8 pills (compared to 13 pills). We save 5,000 pills, which would have cost $45 and also don’t spend the $68 for the creatine; assuming a modafinil formulation, that drops our $1,761 down to $1,648 or $1.65 a day. Or we could remove both the creatine and modafinil, for a grand total of $848 or $0.85 a day, which is pretty reasonable.
…The drugs didn’t work. Or at least only for a bit. “We believed there was no hope without dope but we were wrong. I’m always amazed there aren’t drugs by now, but there aren’t. They didn’t get any better, whereas computers never stopped getting better.”
More than once I have seen results indicating that high-IQ types benefit the least from random nootropics; nutritional deficits are the premier example, because high-IQ types almost by definition suffer from no major deficiencies like iodine. But a stimulant modafinil may be another such nootropic (see “Cognitive effects of modafinil in student volunteers may depend on IQ”, Randall et al 200521ya), which mentions:
Similarly, Mehta et al 2000 noted that the positive effects of methylphenidate (40 mg) on spatial working memory performance were greatest in those volunteers with lower baseline working memory capacity. In a study of the effects of ginkgo biloba in healthy young adults, Stough et al 2001 found improved performance in the Trail-Making Test A only in the half with the lower verbal IQ.
For illustration, consider amphetamines, Ritalin, and modafinil, all of which have been proposed as cognitive enhancers of attention. These drugs exhibit some positive effects on cognition, especially among individuals with lower baseline abilities. However, individuals of normal or above-average cognitive ability often show negligible improvements or even decrements in performance following drug treatment (for details, see de Jongh, Bolt, Schermer, & Olivier, 2008). For instance, Randall, Shneerson, and File (200521ya) found that modafinil improved performance only among individuals with lower IQ, not among those with higher IQ. [See also Finke et al 2010 on visual attention.] Farah, Haimm, Sankoorikal, & Chatterjee 2009 found a similar nonlinear relationship of dose to response for amphetamines in a remote-associates task, with low-performing individuals showing enhanced performance but high-performing individuals showing reduced performance. Such ∩-shaped dose-response curves are quite common (see Cools & Robbins, 2004)
Among other things, these considerations warn us against expecting much from nootropics whose principal justification come from their results in the ill or the old (since we could call being old an illness) - they are already brain-damaged.↩︎
For example, I am have used my Zeo to measure the effects of melatonin or of double-blinded vitamin D on my Zeo sleep data; the latter is novel and interesting.↩︎
I’ve been criticized for calling it “double-blinding”. But if I am both the ‘subject’ and the ‘experimenter’, then blinding one person blinds both roles, and one ought to just call it “blinding”. I believe that “blinding” is ambiguous, though: perhaps I am using a friend or roommate to randomize each dose, in which single-blinding case it is not as good as when I “blind” myself (and achieve a double-blind). The terminology should reflect the true quality of each design, and not conflate single-blinding with double-blinding.↩︎
This is reportedly the result of ‘Ilieva, I., Boland, J., Chatterjee, A. & Farah, M.J. (201016ya). “Adderall’s perceived and actual effects on healthy people’s cognition”. Poster presented at the annual meeting of the Society for Neuroscience, San Diego, CA’; blogger Casey Schwartz describes it:
…researchers have added a new layer to the “smart pill” conversation. Adderall, they’ve found, makes you think you’re doing better than you actually are….Those subjects who had been given Adderall were significantly more likely to report that the pill had caused them to do a better job….But the results of the new University of Pennsylvania study, funded by the U.S. Navy and not yet published but presented at the annual Society for Neuroscience conference last month, are consistent with much of the existing research. As a group, no overall statistically-significant improvement or impairment was seen as a result of taking Adderall. The research team tested 47 subjects, all in their 20s, all without a diagnosis of ADHD, on a variety of cognitive functions, from working memory-how much information they could keep in mind and manipulate-to raw intelligence, to memories for specific events and faces….The last question they asked their subjects was: “How and how much did the pill influence your performance on today’s tests?” Those subjects who had been given Adderall were significantly more likely to report that the pill had caused them to do a better job on the tasks they’d been given, even though their performance did not show an improvement over that of those who had taken the placebo. According to Irena Ilieva…it’s the first time since the 1960s that a study on the effects of amphetamine, a close cousin of Adderall, has asked how subjects perceive the effect of the drug on their performance.
Much better than I had expected. One of the best superhero movies so far, better than Thor or Watchmen (and especially better than the Iron Man movies). I especially appreciated how it didn’t launch right into the usual hackneyed creation of the hero plot-line but made Captain America cool his heels performing & selling war bonds for 10 or 20 minutes. The ending left me a little nonplussed, although I sort of knew it was envisioned as a franchise and I would have to admit that showing Captain America wondering at Times Square is much better an ending than something as cliche as a close-up of his suddenly-opened eyes and then a fade out. (The movie continued the lamentable trend in superhero movies of having a strong female love interest… who only gets the hots for the hero after they get muscles or powers. It was particularly bad in CA because she knows him and his heart of gold beforehand! What is the point of a feminist character who is immediately forced to do that?)↩︎
With just 16 predictions, I can’t simply bin the predictions and say “yep, that looks good”. Instead, we can treat each prediction as equivalent to a bet and see what my winnings (or losses) were; the standard such proper scoring rule is the logarithmic rule which pretty simple: you ‘earn’ the logarithm of the probability if you were right, and the logarithm of the negation if you were wrong; he who racks up the fewest negative points wins. We feed in a list and get back a number:
logScore ps =sum$map (\(result,p) ->if result thenlog p elselog (1-p)) pslogScore [(True,0.95),(False,0.30),(True,0.85),(True,0.75),(False,0.50),(False,0.25), (False,0.60),(True,0.70),(True,0.65),(True,0.60),(False,0.30),(True,0.50), (True,0.90),(True,0.40)]-- -6.125
In this case, a blind guesser would guess 50% every time (roughly half the days were Adderall and roughly half were not) so the question is, did the 50% guesser beat me?
(with 200, 400, 800 and 1600426ya mg) “No effects.”
(with 500 mg) “No effects.”
(with 800 and 1600426ya mg) “No effects.”
(with 25 and 50 mg i.v.) “No effects.”
…It is without activity in man! Certainly not for the lack of trying, as some of the dosage trials that are tucked away in the literature (as abstracted in the “Qualitative Comments” given above) are pretty heavy duty. Actually, I truly doubt that all of the experimenters used exactly that phrase, “No effects”, but it is patently obvious that no effects were found. It happened to be the phrase I had used in my own notes.
…Phenethylamine is intrinsically a stimulant, although it doesn’t last long enough to express this property. In other words, it is rapidly and completely destroyed in the human body. It is only when a number of substituent groups are placed here or there on the molecule that this metabolic fate is avoided and pharmacological activity becomes apparent.
I wasn’t nearly as much of a tea-drinker when I was younger, and one time at camp, a counselor had brought a coffee espresso machine (he was a fan) and would make one for people. I was curious and tried it. I didn’t like it, any more than I liked any other coffee, but presumably because the caffeine content was so high and I was so caffeine-naive, I would swear drinking it caused visual glitches—not fullblown hallucinations, but still alarming to me. Those visual anomalies have never happened since, but I’ve never forgotten. That first experience has always served to remind me that caffeine is a highly psychoactive stimulant, even if I’ve long since tolerated to huge doses of it and no longer notice anything.↩︎
The abuse liability of caffeine has been evaluated.147,148 Tolerance development to the subjective effects of caffeine was shown in a study in which caffeine was administered at 300 mg twice each day for 18 days.148 Tolerance to the daytime alerting effects of caffeine, as measured by the MSLT, was shown over 2 days on which 250 g of caffeine was given twice each day48 and to the sleep-disruptive effects (but not REM percentage) over 7 days of 400 mg of caffeine given 3 times each day.7 In humans, placebo-controlled caffeine-discontinuation studies have shown physical dependence on caffeine, as evidenced by a withdrawal syndrome.147 The most frequently observed withdrawal symptom is headache, but daytime sleepiness and fatigue are also often reported. The withdrawal-syndrome severity is a function of the dose and duration of prior caffeine use…At higher doses, negative effects such as dysphoria, anxiety, and nervousness are experienced. The subjective-effect profile of caffeine is similar to that of amphetamine,147 with the exception that dysphoria/anxiety is more likely to occur with higher caffeine doses than with higher amphetamine doses. Caffeine can be discriminated from placebo by the majority of participants, and correct caffeine identification increases with dose.147 Caffeine is self-administered by about 50% of normal subjects who report moderate to heavy caffeine use. In post-hoc analyses of the subjective effects reported by caffeine choosers versus nonchoosers, the choosers report positive effects and the nonchoosers report negative effects. Interestingly, choosers also report negative effects such as headache and fatigue with placebo, and this suggests that caffeine-withdrawal syndrome, secondary to placebo choice, contributes to the likelihood of caffeine self-administration. This implies that physical dependence potentiates behavioral dependence to caffeine.
Evidence in support of the neuroprotective effects of flavonoids has increased significantly in recent years, although to date much of this evidence has emerged from animal rather than human studies. Nonetheless, with a view to making recommendations for future good practice, we review 15 existing human dietary intervention studies that have examined the effects of particular types of flavonoid on cognitive performance. The studies employed a total of 55 different cognitive tests covering a broad range of cognitive domains. Most studies incorporated at least one measure of executive function/working memory, with nine reporting significant improvements in performance as a function of flavonoid supplementation compared to a control group. However, some domains were overlooked completely (eg. implicit memory, prospective memory), and for the most part there was little consistency in terms of the particular cognitive tests used making across study comparisons difficult. Furthermore, there was some confusion concerning what aspects of cognitive function particular tests were actually measuring. Overall, while initial results are encouraging, future studies need to pay careful attention when selecting cognitive measures, especially in terms of ensuring that tasks are actually sensitive enough to detect treatment effects.
Cocoa flavanols (CF) positively influence physiological processes in ways which suggest that their consumption may improve aspects of cognitive function. This study investigated the acute cognitive and subjective effects of CF consumption during sustained mental demand. In this randomized, controlled, double-blinded, balanced, three period crossover trial 30 healthy adults consumed drinks containing 520 mg, 994 mg CF and a matched control, with a 3-day washout between drinks. Assessments included the state anxiety inventory and repeated 10-min cycles of a Cognitive Demand Battery comprising of two serial subtraction tasks (Serial Threes and Serial Sevens), a Rapid Visual Information Processing (RVIP) task and a ‘mental fatigue’ scale, over the course of 1 h. Consumption of both 520 mg and 994 mg CF significantly improved Serial Threes performance. The 994 mg CF beverage significantly speeded RVIP responses but also resulted in more errors during Serial Sevens. Increases in self-reported ‘mental fatigue’ were significantly attenuated by the consumption of the 520 mg CF beverage only. This is the first report of acute cognitive improvements following CF consumption in healthy adults. While the mechanisms underlying the effects are unknown they may be related to known effects of CF on endothelial function and blood flow.
If we assume the variance of the daily scores are equal and we exclude the hypothesis that fish oil might make scores worse, then we get a smaller p-value:
before <-c(54,69,42,54,44,62,44,35,85,50,44,42,57,65,51,56,42,53,40,47,45,51,57,57,56,76,66,60,46,52,59,48,28,45,43,47,50,40,57,46,33,19,43,58,36,52,44,64)after <-c(55,76,56,55,44,41,44,45,65,70,46,65,46,52,68,52,57,50,64,43,41,50,69,44,47,63,34,57)wilcox.test(before,after,alternative="less")# Wilcoxon rank sum test with continuity correction## data: before and after# W = 570.5, p-value = 0.1381# alternative hypothesis: true location shift is less than 0(mean(after) -mean(before)) /sd(append(before,after)) # the effect size# 0.28
A Bayesian MCMC analysis using the BEST library gives a similar answer - too much overlap, not enough data:
This metric is a little troubling since working memory is trainable and that’s the point of dual n-back - but my own scores have been stagnant for a long time and the blocking should reduce the impact of any very slow linear growth in scores.↩︎
That is, perhaps light of the right wavelength can indeed save the brain some energy by making it easier to generate ATP. Would 15 minutes of LLLT create enough ATP to make any meaningful difference, which could possibly cause the claimed benefits? The problem here is like that of the famous blood-glucose theory of willpower - while the brain does indeed use up more glucose while active, high activity uses up very small quantities of glucose/energy which doesn’t seem like enough to justify a mental mechanism like weak willpower.↩︎
In my last post, I talked about the idea that there is a resource that is necessary for self-control…I want to talk a little bit about the candidate for this resource, glucose. Could willpower fail because the brain is low on sugar? Let’s look at the numbers. A well-known statistic is that the brain, while only 2% of body weight, consumes 20% of the body’s energy. That sounds like the brain consumes a lot of calories, but if we assume a 2,400 calorie/day diet - only to make the division really easy - that’s 100 calories per hour on average, 20 of which, then, are being used by the brain. Every three minutes, then, the brain - which includes memory systems, the visual system, working memory, then emotion systems, and so on - consumes one (1) calorie. One. Yes, the brain is a greedy organ, but it’s important to keep its greediness in perspective… Suppose, for instance, that a brain in a person exerting their willpower - resisting eating brownies or what have you - used twice as many calories as a person not exerting willpower. That person would need an extra one third of a calorie per minute to make up the difference compared to someone not exerting willpower. Does exerting “self control” burn more calories?
Clarke and Sokoloff (199828ya) remarked that although “[a] common view equates concentrated mental effort with mental work…there appears to be no increased energy utilization by the brain during such processes” (p. 664), and “…the areas that participate in the processes of such reasoning represent too small a fraction of the brain for changes in their functional and metabolic activities to be reflected in the energy metabolism of the brain…” (p. 675).
Gibson and Green (200224ya), talking about a possible link between glucose and cognition, wrote that research in the area “…is based on the assumption that, since glucose is the major source of fuel for the brain, alterations in plasma levels of glucose will result in alterations in brain levels of glucose, and thus neuronal function. However, the strength of this notion lies in its common-sense plausibility, not in scientific evidence…” (p. 185).
Lennie (200323ya) concluded that “[t]he brain’s energy consumption does not change with normal variations in mental activity” and that “overall energy consumption is essentially constant” (p. 495).
Messier (200422ya) concluded that it is “unlikely that the blood glucose changes observed during and after a difficult cognitive task are due to increased brain glucose uptake” (p. 39).
Gibson (200719ya), concluded that “task-induced changes in human peripheral blood glucose are unlikely to reflect changes in relevant areas of brain glucose supply” (p. 75).
And in his followup work, “An opportunity cost model of subjective effort and task performance” (discussion). Kurzban seems to have successfully refuted the blood-glucose theory, with few dissenters from commenting researchers. The more recent opinion seems to be that the sugar interventions serve more as a reward-signal indicating more effort is a good idea, not refueling the engine of the brain (which would seem to fit well with research on procrastination).↩︎
This calculation - reaping only 7⁄9 of the naive expectation - gives one pause. How serious is the sleep rebound? In another article, I point to a mice study that sleep deficits can take 28 days to repay. What if the gain from modafinil is entirely wiped out by repayment and all it did was defer sleep? Would that render modafinil a waste of money? Perhaps. Thinking on it, I believe deferring sleep is of some value, but I cannot decide whether it is a net profit.
That it is somewhat valuable is clear if we consider it under another guise. Imagine you received the same salary you do, but paid every day. Accounting systems would incur considerable costs handling daily payments, since they would be making so many more and so much smaller payments, and they would have to know instantly whether you showed up to work that day and all sorts of other details, and the recipients themselves would waste time dealing with all these checks or looking through all the deposits to their account, and any errors would be that much harder to track down. (And conversely, expensive ‘payday loans’ are strong evidence that for poor people, a bi-weekly payment is much too infrequent.) One might draw a comparison to batching or buffers in computers: by letting data pile up in buffers, the computer can then deal with them in one batch, amortizing overhead over many items rather than incurring the overhead again and again. The downside, of course, is that latency will suffer and performance may drop based on that or the items becoming outdated & useless. The right trade-off will depend on the specifics; one would not expect random buffer-sizes to be optimal, but one would have to test and see what works best.
Similarly, we could try applying Nick Bostrom’s reversal test and ask ourselves, how would we react to a virus which had no effect but to eliminate sleep from alternating nights and double sleep in the intervening nights? We would probably grouch about it for a while and then adapt to our new hedonistic lifestyle of partying or working hard. On the other hand, imagine the virus had the effect of eliminating normal sleep but instead, every 2 minutes, a person would fall asleep for a minute. This would be disastrous! Besides the most immediate problems like safely driving vehicles, how would anything get done? You would hold a meeting and at any point, a third of the participants would be asleep. If the virus made it instead 2 hours on, one hour off, that would be better but still problematic: there would be constant interruptions. And so on, until we reach our present state of 16 hours on, 8 hours off. Given that we rejected all the earlier buffer sizes, one wonders if 16:8 can be defended as uniquely suited to circumstances. Is that optimal? It may be, given the synchronization with the night-day cycle, but I wonder; rush hour alone stands as an argument against synchronized sleep - wouldn’t our infrastructure would be much cheaper if it only had to handle the average daily load rather than cope with the projected peak loads? Might not a longer cycle be better? The longer the day, the less we are interrupted by sleep; it’s a hoary cliche about programmers that they prefer to work in long sustained marathons during long nights rather than sprint occasionally during a distraction-filled day, to the point where some famously adopt a 28 hour day (which evenly divides a week into 6 days). Are there other occupations which would benefit from a 20 hour waking period? Or 24 hour waking period? We might not know because without chemical assistance, circadian rhythms would overpower anyone attempting such schedules. It certainly would be nice if one had long time chunks in which could read a challenging book in one sitting, without heroic arrangements.↩︎
As before in the Adderall trial, we use a binary logarithmic proper scoring rule:
logBinaryScore =sum.map (\(result,p) ->if result then1+logBase2 p else1+logBase2 (1-p))logBinaryScore [(True,0.40),(True,0.50),(False,0.65),(False,0.50), (True,0.75),(False,0.40),(False,0.35),(False,0.60)]-- 0.007
Compare 0.007 to the 5.16 I racked up guessing Adderall! My score is essentially 0.↩︎
I don’t understand how Sun can produce any armodafinil, as the armodafinil patents are recent enough that the modafinil loophole shouldn’t apply.↩︎
Specifically, the film is completely unintelligible if you had not read the book. The best I can say for it is that it delivers the action and events one expects in the right order and with basic competence, but its artistic merits are few. It seems generally devoid of the imagination and visual flights of fancy that animated movies 1 and 3 especially (although Mike Darwin disagrees), copping out on standard imagery like a Star Wars-style force field over Hogwarts Castle, or luminescent white fog when Harry was dead and in his head; I was deeply disappointed to not see any sights that struck me as novel and new. (For example, the aforementioned dead scene could have been done in so many interesting ways, like why not show Harry & Dumbledore in a bustling King’s Cross shot in bright sharp detail, but with not a single person in sight and all the luggage and equipment animatedly moving purposefully on their own?) The ending in particular boggles me. I actually turned to the person next to me and asked them whether that really was the climax and Voldemort was dead, his death was so little dwelt upon or laden with significance (despite a musical score that beat you over the head about everything else). In the book, I remember it feeling like a climactic scene, with everyone watching and little speeches explaining why Voldemort was about to be defeated, and a suitable victory celebration; I read in the paper the next day a quote from the director or screenwriter who said one scene was cut because Voldemort would not talk but simply try to efficiently kill Harry. (This is presumably the explanation for the incredible anti-climax. Hopefully.) I was dumbfounded by the depths of dishonesty or delusion or disregard: Voldemort not only does that in Deathly Hallows multiple times, he does it every time he deals with Harry, exactly as the classic villains (he is numbered among) always do! How was it possible for this man to read the books many times, as he must have, and still say such a thing?↩︎
This was using Brain Workshop, D5B, 45 trials over 157 seconds.↩︎
…Four subjects correctly stated when they received nicotine, five subjects were unsure, and the remaining two stated incorrectly which treatment they received on each occasion of testing. These numbers are sufficiently close to chance expectation that even the four subjects whose statements corresponded to the treatments received may have been guessing.
As I see you didn’t control for the training effect of dual-n-back. Are your dual-n-back scores generally stable enough that you don’t have a strong training effect anymore?
I don’t believe there’s any need to control for training with repeated within-subject sampling, since there will be as many samples on both control and active days drawn from the later “trained” period as with the initial “untrained” period. But yes, my D5B scores seem to have plateaued pretty much and only very slowly increase; you can look at the stats file yourself.
But to investigate, let’s look a graph of my last ~200 D5B scores:
231 dual 5-back scores plotted in chronological order: plot(dnb)
The point about randomization is key, BTW, because the theoretical training effect is actually greater than the observed improvement between randomized days. Watch:
lm(dnb ~c(1:231))# Coefficients:# (Intercept) c(1:231)# 38.37041 0.01752## 0.017 is a positive slope!
DNB scores per day with a linear fit overlaid; plot(dnb); abline(lm(dnb ~ c(1:231)))
It’s not much of a slope but it’s there. Now, I spent 200 rounds of n-back doing the randomized nicotine experiment, and those would be the latter 200 rounds graphed; how much of an improvement should I expect?
The model is: y=38.37041+0.01752⋅x. We want the endpoint, score 231, and what is 200 before 231? 31:
That study is also interesting for finding benefits to chronic piracetam+choline supplementation in the mice, which seems connected to a Russian study which reportedly found that piracetam (among other more obscure nootropics) increased secretion of BDNF in mice. See also Drug heuristics on a study involving choline supplementation in pregnant rats.↩︎
We do a one-tailed test because the original hypothesis was that M/P would fall, certainly not that it would increase:
wilcox.test(poff,c(pone,ptwo), alternative="less")# Wilcoxon rank sum test with continuity correction## data: poff and c(pone, ptwo)# W = 593, p-value = 0.1502
One might expect some sort of catch - surely there’s a massive quality difference to go with the massive price difference? But there could well not be; I would not be surprised to learn that the dog selegiline and the human selegiline came out of the same vat.
It’s basic economics: the price of a good must be greater than cost of producing said good, but only under perfect competition will price = cost. Otherwise, the price is simply whatever maximizes profit for the seller. (Bottled water doesn’t really cost $2 to produce.) This can lead to apparently counter-intuitive consequences involving price discrimination & market segmentation - such as ‘damaged’ goods which are the premium product which has been deliberately degraded and sold for less (some Intel CPUs, some headphones etc.). The most famous examples were railroads; one notable passage by French engineer-economist Jules Dupuit describes the motivation for the conditions in 1849177ya:
It is not because of the few thousand francs which would have to be spent to put a roof [!] over the third-class carriages or to upholster the third-class seats that some company or other has open carriages with wooden benches. What the company is trying to do is to prevent the passengers who can pay the second class fare from traveling third class; it hits the poor, not because it wants to hurt them, but to frighten the rich. And it is again for the same reason that the companies, having proved almost cruel to the third-class passengers and mean to the second-class ones, become lavish in dealing with first-class passengers. Having refused the poor what is necessary, they give the rich what is superfluous.
Price discrimination is aided by barriers such as ignorance and oligopolies. An example of the former would be when I went to a Food Lion grocery store in search of spices, and noticed that there was a second selection of spices in the “Hispanic/Latino” ethnic food aisle, with unit prices perhaps a fourth of the regular McCormick-brand spices; I rather doubt that regular cinnamon varies that much in quality. An example of the latter would be using veterinary drugs on humans - any doctor to do so would probably be guilty of medical malpractice even if the drugs were manufactured in the same factories (as well they might be, considering economies of scale). Similarly, we can predict that whenever there is a veterinary drug which is chemically identical to a human drug, the veterinary drug will be much cheaper, regardless of actual manufacturing cost, than the human drug because pet owners do not value their pets more than themselves. Human drugs are ostensibly held to a higher standard than veterinary drugs; so if veterinary prices are higher, then there will be an arbitrage incentive to simply buy the cheaper human version and ‘downgrade’ them to veterinary drugs.
As with any thesis, there are exceptions to this general practice. For example, theanine for dogs is sold under the brand Anxitane is sold at almost a dollar a pill, and apparently a month’s supply costs $50+ vs $13 for human-branded theanine; on the other hand, this thesis predicts ‘downgrading’ if the market priced pet versions higher than human versions, and that Reddit poster appears to be doing just that with her dog.↩︎
It’s important one uses D-3 and not vitamin D-2, alfacalcidol, or calcitriol: the Cochrane review found mortality benefits only with D-3. (And use with calcium doesn’t look too good either.)↩︎
It’s been suggested that caffeine interferes with production or absorption of vitamin D and this may be a bad thing; eg. Medpedia or blogger Chris Hunt (HN discussion):
Caffeine keeps you awake, which keeps you coding. It may also be a nootropic, increasing brain-power. Both desirable results. However, it also inhibits vitamin D receptors, and as such decreases the body’s uptake of this-much-needed-vitamin. OK, that’s not so bad, you’re not getting the maximum dose of vitamin D. So what? Well, by itself caffeine may not cause you any problems, but combined with cutting off a major source of the vitamin - the production via sunlight - you’re leaving yourself open to deficiency in double-quick time.
Too much caffeine may be bad for bone health because it can deplete calcium. Overdoing the caffeine also may affect the vitamin D in your body, which plays a critical role in your body’s bone metabolism. However, the roles of vitamin D as well as caffeine in the development of osteoporosis continue to be a source of debate. Significance: Caffeine may interfere with your body’s metabolism of vitamin D, according to a 200719ya “Journal of Steroid Biochemistry & Molecular Biology” study. You have vitamin D receptors, or VDRs, in your osteoblast cells. These large cells are responsible for the mineralization and synthesis of bone in your body. They create a sheet on the surface of your bones. The D receptors are nuclear hormone receptors that control the action of vitamin D-3 by controlling hormone-sensitive gene expression. These receptors are critical to good bone health. For example, a vitamin D metabolism disorder in which these receptors don’t work properly causes rickets.
Caffeine dose dependently decreased the 1,25(OH)(2)D(3) induced VDR expression and at concentrations of 1 and 10mM, VDR expression was decreased by about 50-70%, respectively. In addition, the 1,25(OH)(2)D(3) induced alkaline phosphatase activity was also reduced at similar doses thus affecting the osteoblastic function. The basal ALP activity was not affected with increasing doses of caffeine. Overall, our results suggest that caffeine affects 1,25(OH)(2)D(3) stimulated VDR protein expression and 1,25(OH)(2)D(3) mediated actions in human osteoblast cells.
One should note the serious caveats here: it is a small in vitro study of a single category of human cells with an effect size that is not clear on a protein which feeds into who-knows-what pathways. It is not a result in a whole organism on any clinically meaningful endpoint, even if we take it at face-value (many results never replicate). A look at followup work citing Rapuri et al 200719ya is not encouraging: Google Scholar lists no human studies of any kind, much less high-quality studies like RCTs; just some rat followups on the calcium effect. This is not to say Rapuri et al 200719ya is a bad study, just that it doesn’t bear the weight people are putting on it: if you enjoy caffeine, this is close to zero evidence that you should reduce or drop caffeine consumption; if you’re taking too much caffeine, you already have plenty of reasons to reduce; if you’re drinking lots of coffee, you already have plenty of reasons to switch to tea; etc.
If we go looking for meaningful human studies, what we find is that there’s clear evidence that caffeine damages bone density via calcium uptake, especially in old women, but there is little or no interaction between vitamin D and caffeine, and some reports of correlations entirely opposite the claimed correlation.
Results: Women with high caffeine intakes had significantly higher rates of bone loss at the spine than did those with low intakes (−1.90 ± 0.97% compared with 1.19 ± 1.08%; P = 0.038). When the data were analyzed according to VDR genotype and caffeine intake, women with the tt genotype had significantly (P = 0.054) higher rates of bone loss at the spine (−8.14 ± 2.62%) than did women with the TT genotype (−0.34 ± 1.42%) when their caffeine intake was >300 mg/d…In 199432ya, Morrison et al (22) first reported an association between vitamin D receptor gene (VDR) polymorphism and BMD of the spine and hip in adults. After this initial report, the relation between VDR polymorphism and BMD, bone turnover, and bone loss has been extensively evaluated. The results of some studies support an association between VDR polymorphism and BMD (23-,25), whereas other studies showed no evidence for this association (26,27)…At baseline, no significant differences existed in serum parathyroid hormone, serum 25-hydroxyvitamin D, serum osteocalcin, and urinary N-telopeptide between the low- and high-caffeine groups (Table 1⇑). In the longitudinal study, the percentage of change in serum parathyroid hormone concentrations was significantly lower in the high-caffeine group than in the low-caffeine group (Table 2⇑). However, no significant differences existed in the percentage of change in serum 25-hydroxyvitamin D
In simple and multiple regression analyses, the only significant variable that affected Ad-SOS and nutrient intake was vitamin D (p < 0.0001). Phalangeal bone Ad-SOS was influenced only by the intake of vitamin D, not of caffeine or other nutrients.
In this large population-based cohort, we saw consistent robust associations between cola consumption and low BMD in women. The consistency of pattern across cola types and after adjustment for potential confounding variables, including calcium intake, supports the likelihood that this is not due to displacement of milk or other healthy beverages in the diet. The major differences between cola and other carbonated beverages are caffeine, phosphoric acid, and cola extract. Although caffeine likely contributes to lower BMD, the result also observed for decaffeinated cola, the lack of difference in total caffeine intake across cola intake groups, and the lack of attenuation after adjustment for caffeine content suggest that caffeine does not explain these results. A deleterious effect of phosphoric acid has been proposed (26). Cola beverages contain phosphoric acid, whereas other carbonated soft drinks (with some exceptions) do not.
Compared with those reporting no use, subjects drinking >4 cups/day of decaffeinated coffee were at increased risk of RA [rheumatoid arthritis] (RR 2.58, 95% CI 1.63-4.06). In contrast, women consuming >3 cups/day of tea displayed a decreased risk of RA (RR 0.39, 95% CI 0.16-0.97) compared with women who never drank tea. Caffeinated coffee and daily caffeine intake were not associated with the development of RA.
Since coffee drinking may lead to a worsening of calcium balance in humans, we studied the serial changes of serum calcium, PTH, 1,25-dihydroxyvitamin D (1,25(OH)2D) vitamin D and calcium balance in young and adult rats after daily administration of caffeine for 4 weeks. In the young rats, there was an increase in urinary calcium and endogenous fecal calcium excretion after four days of caffeine administration that persisted for the duration of the experiment. Serum calcium decreased on the fourth day of caffeine administration and then returned to control levels. In contrast, the serum PTH and 1,25(OH)2D remained unchanged initially, but increased after 2 weeks of caffeine administration…In the adult rat group, an increase in the urinary calcium and endogenous fecal calcium excretion and serum levels of PTH was found after caffeine administration. However, the serum 1,25(OH)2D levels and intestinal absorption coefficient of calcium remained the same as in the adult control group.
The addition of body mass index, physical activity, calcium intake, and alcohol consumption to the regression model raised the effect estimate slightly. The further addition of vitamin D, protein, and caffeine intakes had little effect on the results.
A total of 330 randomly selected Saudi adolescents were included. Anthropometrics were recorded and fasting blood samples were analyzed for routine analysis of fasting glucose, lipid levels, calcium, albumin and phosphorous. Frequency of coffee and tea intake was noted. 25-hydroxyvitamin D levels were measured using enzyme-linked immunosorbent assays…Vitamin D levels were significantly highest among those consuming 9-12 cups of tea/week in all subjects (p-value 0.009) independent of age, gender, BMI, physical activity and sun exposure.
Although there have been large trials with the elderly using much higher Vitamin D doses, such as 4 doses every year of 100,000 IU, or a single annual dose of up to 300,000 IU without observed problems.↩︎
{kind=link}



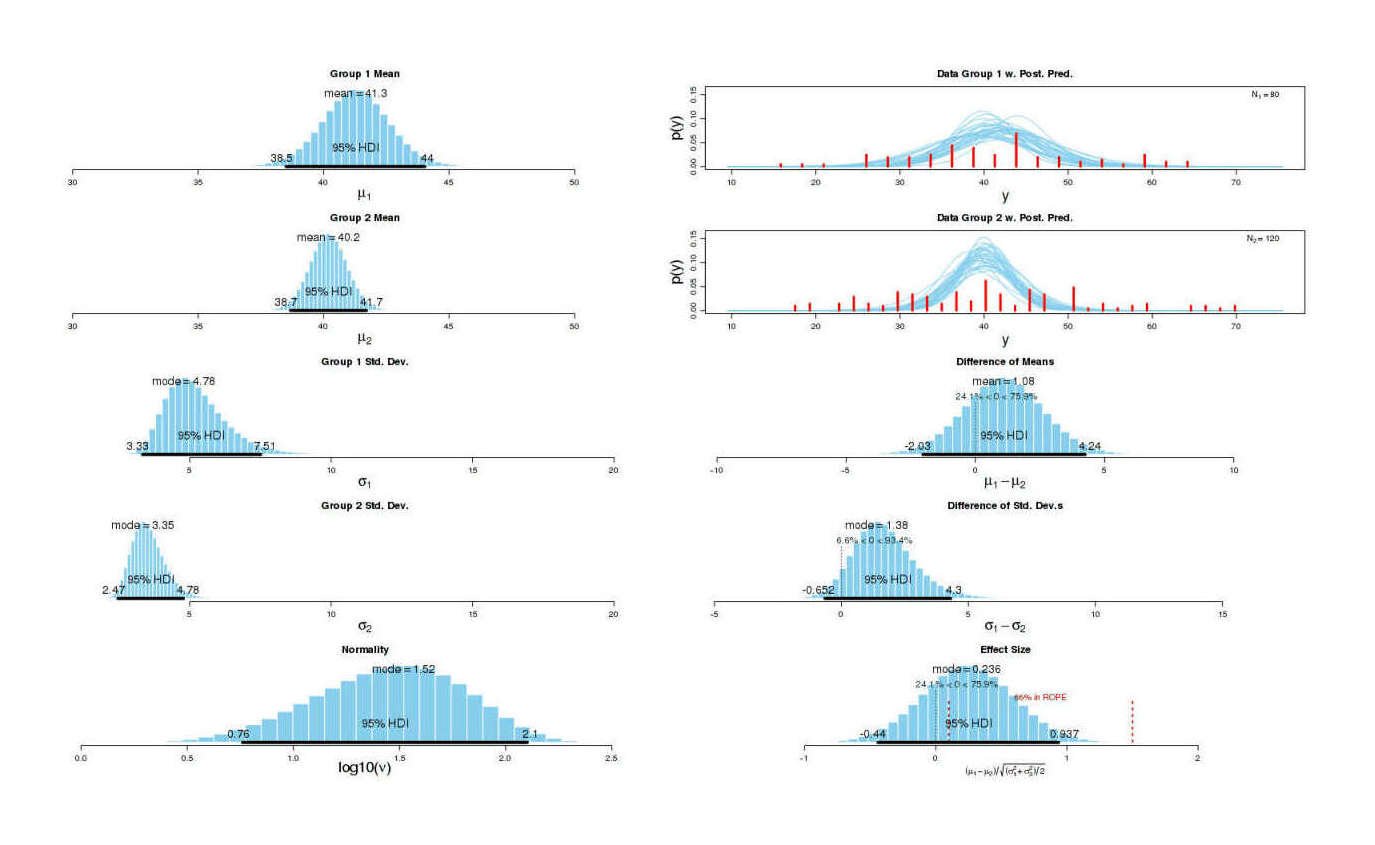
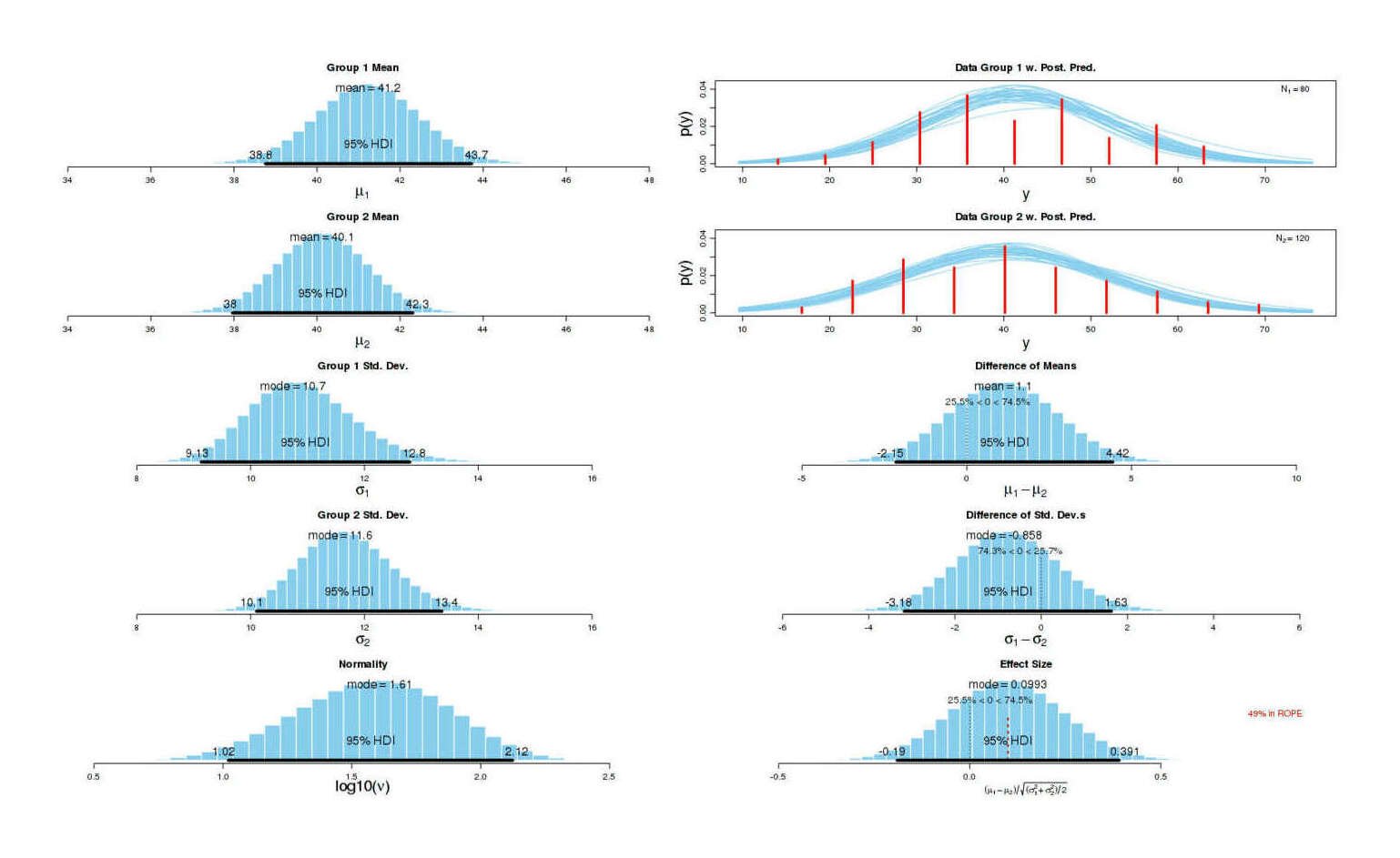
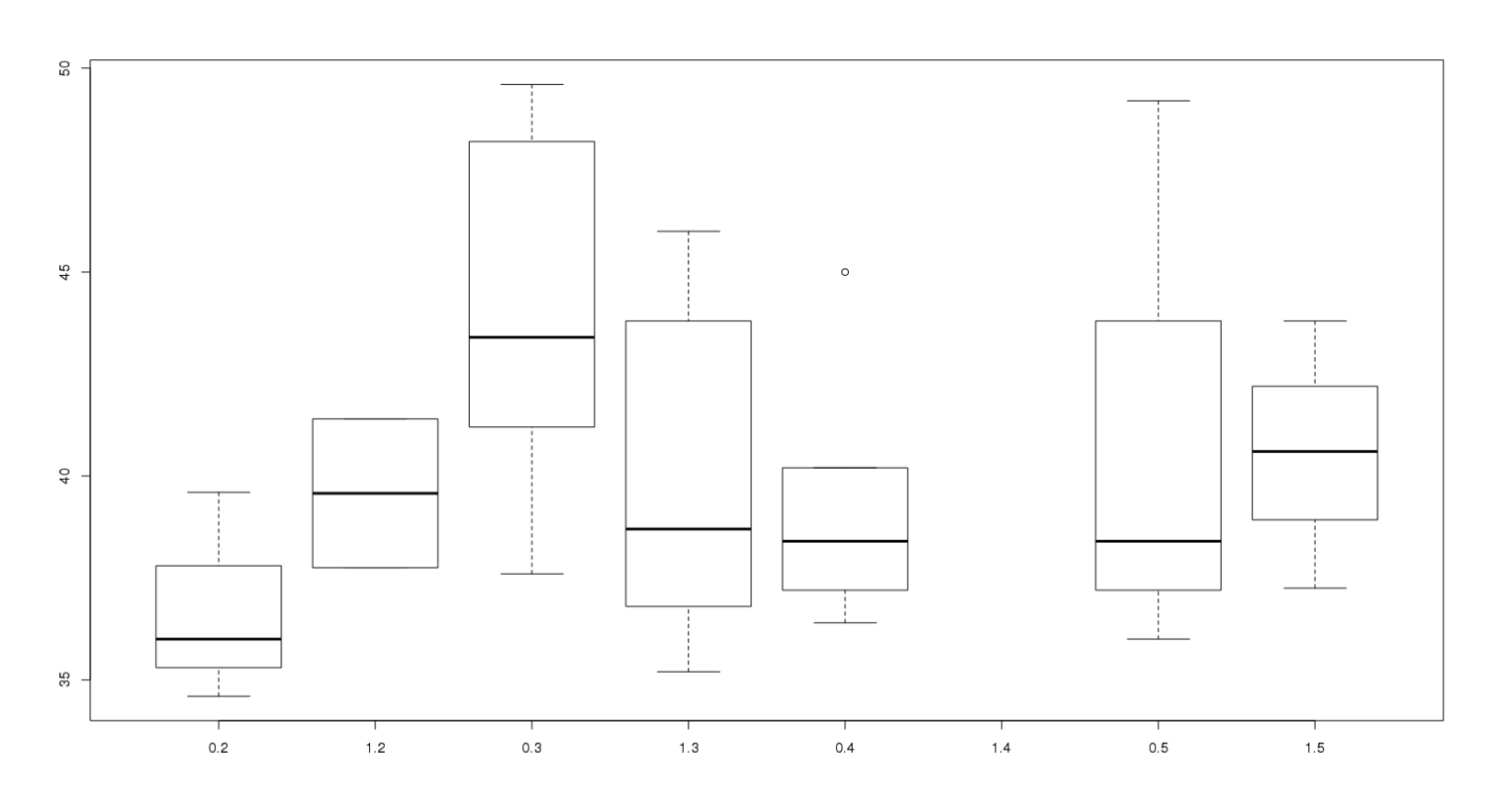

{kind=link}
{kind=link}

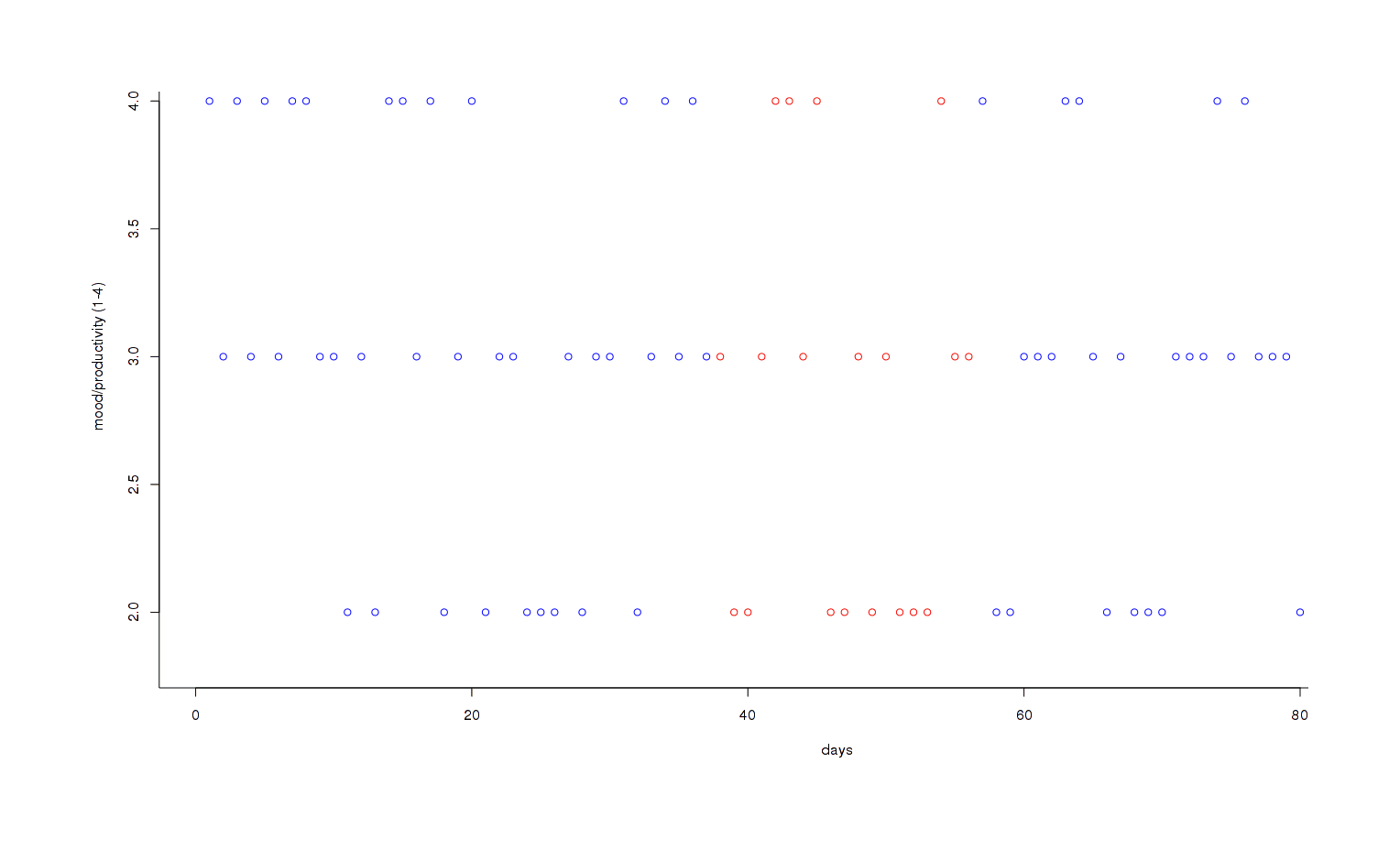
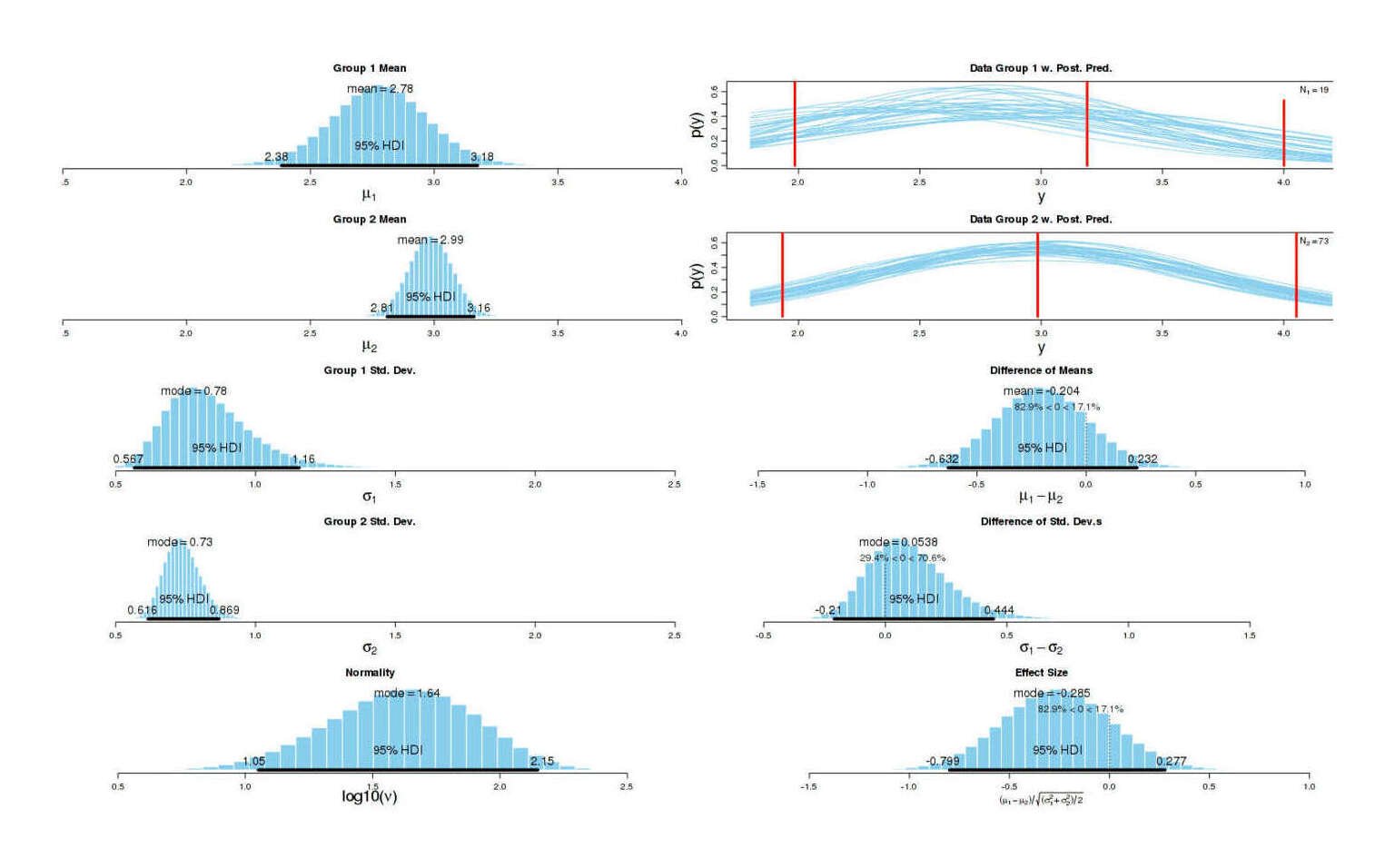
{kind=link}