The Conversation (3)
Sort by

The dominant player in the robotic surgery industry is Intuitive Surgical, which has more than 6,700 da Vinci machines in hospitals around the world. The robot’s four arms can all be controlled by a single surgeon.
Before the robots arrived, surgical training was done the same way for nearly a century.
During routine surgeries, trainees worked with nurses, anesthesiologists, and scrub technicians to position and sedate the patient, while also preparing the surgical field with instruments and lights. In many cases, the trainee then made the incision, cauterized blood vessels to prevent blood loss, and positioned clamps to expose the organ or area of interest. That’s often when the surgeon arrived, scrubbed in, and took charge. But operations typically required four hands, so the trainee assisted the senior surgeon by suctioning blood and moving tissue, gradually taking the lead role as he or she gained experience. When the main surgical task was accomplished, the surgeon scrubbed out and left to do the paperwork. The trainee then did whatever stitching, stapling, or gluing was necessary to make the patient whole again.
In that old system, trainees were in charge for several hours of each procedure. It wasn’t much different for laparoscopic surgery (sometimes called “minimally invasive surgery”), in which tools and cameras are put into the patient via tiny slits. In those surgeries, trainees did much of the preliminary work and cleanup as well. This system of master-apprentice cooperation was so entrenched that hours spent in the operating room (OR) are still seen as a proxy for skill development.
That’s not working in robotic surgery. Surgical robots have become increasingly prevalent in hospitals ever since the da Vinci Surgical System was approved by the U.S. Food and Drug Administration in 2000. The da Vinci robot, from the Silicon Valley–based company Intuitive Surgical, dominates the market today. Intuitive has more than 6,700 machines in hospitals around the world, and the company says that in the United States, da Vinci machines are used in 100 percent of top-rated hospitals for cancer, urology, gynecology, and gastroenterology diseases. There are also a variety of specialized robotic systems from other companies that are used in fields such as orthopedics, neurology, and ophthalmology.
In robotic surgeries, the most dangerous times are at the beginning and the end, when the surgical team “docks” the massive robot to the patient. For the current generation of da Vinci systems, that means positioning four robotic arms tipped with surgical tools and creating “ports” for those tools by inserting metal cylinders into the patient’s abdomen via small incisions. The first port allows the entry of the camera; the ports are used for scalpels, graspers, cauterizing instruments, staplers, or other tools.
Once the robotic arms are in place and instruments are inserted, the surgeon “scrubs out” and takes up position perhaps 15 feet away from the patient in the immersive da Vinci control console, which provides a stereoscopic view. The surgeon’s hands are on two multipurpose controllers that can move and rotate the instruments in all directions; by switching between instruments, the surgeon’s two hands can easily control all four robotic arms.
And the trainee… well, the trainee gets to watch from another console, if there is one. While the lead surgeon could theoretically give the trainee one of the robot arms to control, in practice it never happens. And surgeons are reluctant to give the trainee control over all the arms because they know that will make the procedure take longer, and the risk to the patient goes up nonlinearly with elapsed time under anesthesia.
I began researching the impact of surgical robots on surgical technique and education in 2013. My studies have found that hospitals that adopted the technology have most often turned trainees into optional assistants in the OR, meaning that they begin practicing as “real” surgeons without enough skill. Reversing this trend would require sweeping institutional change, which I don’t expect to happen anytime soon. So, I’m working with collaborators on an alternate solution for surgical skill learning. The platform we create could turn out to be broadly useful, perhaps even turning into a blueprint for 21st-century apprenticeship.
Surgical robots are marvels of engineering in many ways. The da Vinci system gives surgeons a magnified view and robotic hands that never shake, enabling very precise surgical maneuvers. It also provides more efficient and intuitive control than surgeons get from laparoscopic tools: Those operate on fulcrums, so moving a hand to the left moves the tool to the right. The da Vinci robot also provides haptic feedback, with earlier models vibrating the controllers if the software detected instrument “clashes,” and more recent models providing similar feedback when surgeons move too quickly or operate out of the visual field. And the ergonomic consoles are certainly easier on surgeons’ bodies; they no longer have to hunch over an operating table for hours at a time. The robots have also been a marketing phenomenon that has led to a robotic-surgery arms race, with mid-tier hospitals advertising their high-tech capabilities.
Many people assume that patient outcomes must be better with robotic surgery. It’s not obvious that’s true. In fact, a recent survey of 50 randomized control trials that compared robotic surgery to conventional and laparoscopic surgeries found that outcomes were comparable, and robotic surgeries were actually a bit slower. From my perspective, focusing on education, it’s something of a miracle that outcomes aren’t worse, given that residents are going to their first jobs without the necessary experience. It may be that the outcomes of inexperienced junior surgeons are counterbalanced by those of senior surgeons—or it may be that junior surgeons are really learning on their first patients “in the wild,” which is a somewhat uncomfortable idea. This is a hot research area, so we should know more soon.
It may seem counterintuitive that surgical trainees need more training time. To become a surgeon, a person must first spend four years in medical school and then at least five years in a residency program. Medical residents are famously overworked and sleep-deprived, to the extent that the United States passed regulations in 2003 limiting their workweek to 80 hours. But although surgical residents spend many hours in the OR, my findings show that those hours aren’t giving them the skills they need. And because they’re always racing from one patient-related task to the next, they spent almost no time on simulator programs, though they are available. The last time I checked on this situation, about a year ago, most hospitals mandated that residents spend about four hours per year on simulators. That’s like asking someone to play a video game for four hours per year to prepare for a life-or-death situation.
In many ways, the issues arising in robotic surgery mirror those confronted by other professions as they have come to rely increasingly on automation. The situation is summed up as the “ automation paradox”: The more advanced and reliable the automated system, the more crucial the contributions of the human operator. That’s because the system will inevitably encounter unexpected circumstances that fall outside its design parameters or will fail in some way. In those rare but critical moments, the operator must detect the failure and take over, quickly bringing the very human faculties of creativity and problem solving to bear on a tricky situation. Airline pilots became familiar with this issue as autopilot became ubiquitous, and the promise of self-driving cars is bringing this conversation to the general public. Surgical robots have quite limited autonomy at this point, so the surgical profession should learn from these examples and act now, changing the human-machine relationship to both preserve surgical skill and avert tragic crashes in the OR.
My conclusions come from two years spent studying the impact of robots on surgical training. I spent a great deal of time at five hospitals, observing 94 surgeries that took a total of 478 hours. I next conducted interviews at 13 more top-tier teaching hospitals around the United States, gathering information from senior surgeons and sets of trainees that the surgeons deemed high-performing or average. The paper I published in 2019 summarized my findings, which were dismaying. The small subset of trainees who succeeded in learning the skills of robotic surgery did so for one of three reasons: They specialized in robotics at the expense of everything else, they spent any spare minutes doing simulator programs and watching YouTube videos, or they ended up in situations where they performed surgeries with little supervision, struggling with procedures that were at the edge of their capabilities. I call all these practices “shadow learning,” as they all bucked the norms of medical education to some extent. I’ll explain each tactic in more detail.
Residents who engaged in “premature specialization” would begin, often in medical school and sometimes earlier, to give short shrift to other subjects or their personal lives so they could get robotics experience. Often, they sought out research projects or found mentors who would give them access. Losing out on generalist education about medicine or surgery may have repercussions for trainees. Most obviously, there are situations where surgeons must turn off the robots and open up the patient for a hands-on approach. That situation almost never occurs because of a robotic failure; it’s more likely to occur if something goes wrong during the robotic procedure. If the surgeon accidently nicks a vein or cuts through a tumor in a way that causes a leakage of cancerous cells, the recovery mode is to undock the robot rapidly, cut the patient open, and fix the problem the old-fashioned way. My data strongly suggest that residents who prematurely specialize in robotics will not be adequately prepared to handle such situations.
The robots are a marketing phenomenon that has led to a robotic-surgery arms race, with mid-tier hospitals advertising their high-tech capabilities.
The second practice of successful trainees was abstract rehearsal, spending their spare moments in simulators and carefully reviewing surgical videos. One resident told me that he watched a one-hour video of a certain procedure perhaps 200 times to understand every part of it. But passively watching videos only helped so much. Many recordings had been made public because they were particularly good examples of a procedure, for example. In other words, they were procedures where nothing went wrong.
Practicing on the simulator was helpful for trainees, giving them fluency in the basics of robotic control that might impress a senior surgeon in the OR and cause the trainee to get more time on the console. But in the case of the da Vinci system, the simulator software was often only available via the real console, so residents could only practice with it when an OR was empty—which typically meant staying at the hospital into the evening. A few elite institutions had simulation centers, but these were often some distance from the hospital. Most residents didn’t shirk other responsibilities to make the time for such dedicated practice.
An additional drawback of the simulators, some senior surgeons told me, was that they don’t include enough examples of the myriad and compounding ways in which things can go wrong during surgery. Even the best surgeons make errors, but they recover from them: For example, a surgeon might accidentally nick a small blood vessel with a scalpel but quickly seal the cut and move on. In surgery and many other occupations, one of the most important things that trainees need to learn is how to make errors and recover from them.
The final practice of successful trainees was finding situations in which they were able to operate on a patient with little supervision, often working near the edge of their competency and often in violation of hospital policies. Some were working under “superstar” surgeons who were officially in charge of several simultaneous procedures, for example. In such cases, the expert would swoop in only for the trickiest part of each operation. Others rotated from high-status hospitals to departments or hospitals that had relatively little experience with robotic surgery, making the trainees seem competent and trustworthy. Middle-tier hospitals also put less pressure on surgeons to get procedures done quickly, so handing control to a trainee, which inevitably slows things down, was seen as more acceptable. Residents in all these situations were often tense and nervous, they told me, but their struggle was the source of their learning.
To change this situation in a systematic way would require overhauling surgical residency programs, which doesn’t seem likely to happen anytime soon. So, what else can be done?
Intuitive has more than 6,700 machines in hospitals around the world; in the United States, Intuitive says that da Vinci machines are used in 100 percent of top-rated hospitals for cancer, urology, gynecology, and gastroenterology diseases.
In the past five years, there has been an explosion of apps and programs that enable digital rehearsal for surgical training (including both robotic techniques and others). Some, like Level EX and Orthobullets, offer quick games to learn anatomy or basic surgical moves. Others take an immersive approach, leveraging recent developments in virtual reality like the Oculus headset. One such VR system is Osso VR, which offers a curriculum of clinically accurate procedures that a trainee can practice in any location with a headset and Wi-Fi.
I’m working on something different: a collaborative learning process for surgical skill that I hope could be analogous to GitHub, the platform for hosting open-source software. On GitHub, a developer can post code, and others can build on it, sometimes disagreeing about the best way forward and creating branching paths. My collaborator Juho Kim and I are in the early stages of building a crowdsourced repository for annotated and annotatable surgical videos, not only eliminating the time required to search for useful videos on YouTube but also giving watchers a way to interact with the video and increase their active learning. Thankfully, we have a superb industry collaborator as well: the Michigan Urological Surgery Improvement Collaborative. They curate an open library of robotic urologic surgical videos that is known worldwide.
One somewhat similar platform exists for video-based learning: the C-SATS platform, which is now a subsidiary of Johnson & Johnson. That subscription-based platform enables surgeons to securely upload their own videos and uses AI to scrub out all personally identifying information, such as images of a patient’s face. It then gives surgeons personalized feedback on their performance.
If C-SATS is the Encyclopedia Britannica, we’ll be Wikipedia. We’re currently testing an alpha version of our free and open-source platform, which we call Surch. Recently, we’ve been testing an alpha version with groups of surgeons and residents at select top-tier teaching hospitals to determine which features would be the most valuable to them. We’ve asked testers to complete tasks they typically struggle with: finding good quality surgical videos that match their learning objectives, processing videos actively by making notes on things like surgical phases and anatomy, and sharing those notes with others for feedback. It’s still an academic project, but based on the enthusiastic response we’ve gotten from testers, there seems to be demand for a commercial product. We may try to embed it in a surgical residency program for a year to test the platform further.
I believe that we need a 21st-century infrastructure for apprenticeship.
I believe that we need a 21st-century infrastructure for apprenticeship. The problems I found in robotic skill development have arisen because surgeons are relying on an apprenticeship model that was invented many thousands of years ago: Watch an expert for a while, get increasingly involved, then start to help more junior members along. This process goes by many names—in surgery, it’s called “see one, do one, teach one”—but it always requires one-on-one collaboration in real work, and it’s therefore not remotely scalable.
Since the 1990s, our societies have invested heavily in the infrastructure needed to scale formal learning of explicit knowledge; think of the proliferation of online lectures, documents, quizzes, group chats, and bulletin boards. We need the equivalent infrastructure for embodied skill if we’re going to build the capabilities we need for new kinds of work.
My collaborators and I imagine our Surch platform evolving into an AI-enabled global GitHub for skill learning. Any form of procedural knowledge could be captured, studied, and shared on this kind of platform—supported by AI, people could efficiently and collaboratively learn how to shuck oysters, remove tree stumps, change the oil in their cars, and countless other tasks. Of course, we’ll be grateful and excited if our system makes a difference just for surgeons. But the world requires many skills that you can’t write down, and we need to find a modern way to keep these capabilities alive.


The Internet of Things, with technologies such as sensors, microcontrollers, actuators, and connectivity modules together with security solutions and software, has great potential to prevent diseases and improve health.
Technology, and with it the Internet of Things (IoT) has the potential to support the healthcare sector across all levels, for example with predictive prevention and monitoring, in diagnosis and treatment as well as in follow-up care and support in daily life.
There are numerous health and fitness devices able to track key health markers, such as a user’s heart rate or breathing patterns, that may afford users greater awareness of their health and allow them to make pro-active decisions regarding their health and well-being.
Infineon Technologies
The global IoT market trend in medical devices is clearly moving towards “healthcare is self-care” with a focus on active patient engagement and patient-centric care. The vital signs monitoring segment is expected to grow at the highest rate.
Let’s take smart health devices like fitness wearables as an example: A medical band tracks health and fitness data and enables an efficient monitoring for individuals, doctors, and medical staff. Particularly valuable in critical situations: In the event of conspicuous irregularities, the medical band can advise users to take a certain action first, for example, taking a medication. If serious irregularities develop, the doctor can be contacted or an emergency call can be triggered.
Infineon’s semiconductor products and software solutions are the perfect match for smart health devices as they meet the needs of digital healthcare applications. We support a health-conscious lifestyle by enabling smart devices that can help improve well-being and stay healthy longer by making them reliable, convenient, personalized — and secure. That’s our contribution to a functioning healthcare system facing a rising global population and aging.
But there are also smart health devices that do not have to be worn on the body, as the example of smart health monitoring solutions for the home shows. The increase in chronic diseases and health problems in our society often entails the need for home care or self-treatment at home. The desire for a self-determined life is just as decisive for this as the lack of suitable facilities in some regions.
This is where the smart home can help with home automation and health monitoring solutions like sleep monitors based on radar technology that are so small and easy to use that they can replace examinations in the artificial environment of a sleep laboratory. Patients can record their sleeping behavior with high precision at home, without external stress factors, in a familiar environment – even when covered by bedding.
The use of digital technologies in health and lifestyle has advanced exponentially. This increase in digitalization makes the safeguarding of health and patient data urgent and is a basic requirement for the functioning of the digital health system. With topics such as Artificial Intelligence (AI), Machine Learning (ML) and Big Data also playing an increasingly important role, it is becoming essential to secure data to prevent the misuse of private and sensitive information.
Equipping smart health devices with the right security solutions from the get-go is key to helping prevent attacks – whether theft, fraud or manipulation. Companies that are looking for a security solution need one that is equally easy to use – in terms of fast integration and time to market – and trustworthy. Unlike software-only solutions a hardware-based solution is strong, tamperproof and provides a solid foundation.
Semiconductors from companies like Infineon are essential components in all solutions as they support the design of innovative technologies and devices for health-monitoring, preventive healthcare like sleep monitoring and, in the event of illness, self-treatment and assisted living at home. Sensors record vital data, microcontrollers process and forward it, actuators trigger actions, networking technologies integrate cloud services with medical expertise, and security solutions ensure the protection of extremely sensitive personal data.
1) United Nations Department of Economic and Social Affairs, Population Division (2022): World Population Prospects 2022: Summary of Results. UN DESA/POP/2022/TR/NO. 3.


Dead, and in a jacket and tie. That’s how he was on 1 December 1948, when two men found him slumped against a retaining wall on the beach at Somerton, a suburb of Adelaide, Australia.

Police distributed a photograph, but no one came forward to claim the body. Eyewitnesses reported having seen the man, whom the newspapers dubbed the Somerton Man and who appeared to be in his early 40s, lying on the beach earlier, perhaps at one point moving his arm, and they had concluded that he was drunk. The place of death led the police to treat the case as a suicide, despite the apparent lack of a suicide note. The presence of blood in the stomach, a common consequence of poisoning, was noted at the autopsy. Several chemical assays failed to identify any poison; granted, the methods of the day were not up to the task.
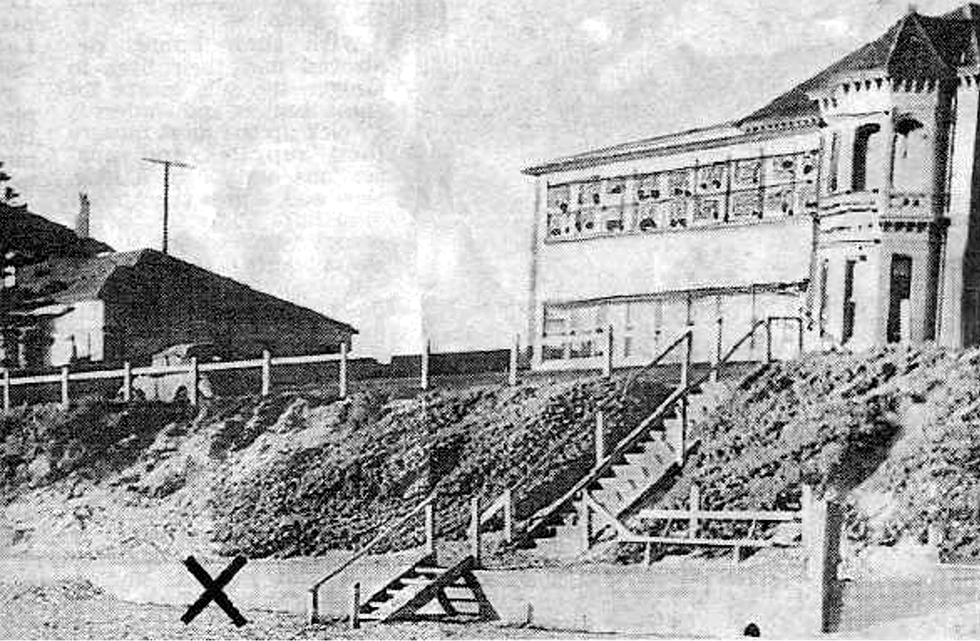 The place on Somerton Beach where the man was found dead is marked with an X.
NEWS CORP./ALAMY
The place on Somerton Beach where the man was found dead is marked with an X.
NEWS CORP./ALAMY
 Policemen recovered the man’s suitcase from the Adelaide city railway station and examined its contents.
NEWS CORP./ALAMY
Policemen recovered the man’s suitcase from the Adelaide city railway station and examined its contents.
NEWS CORP./ALAMY
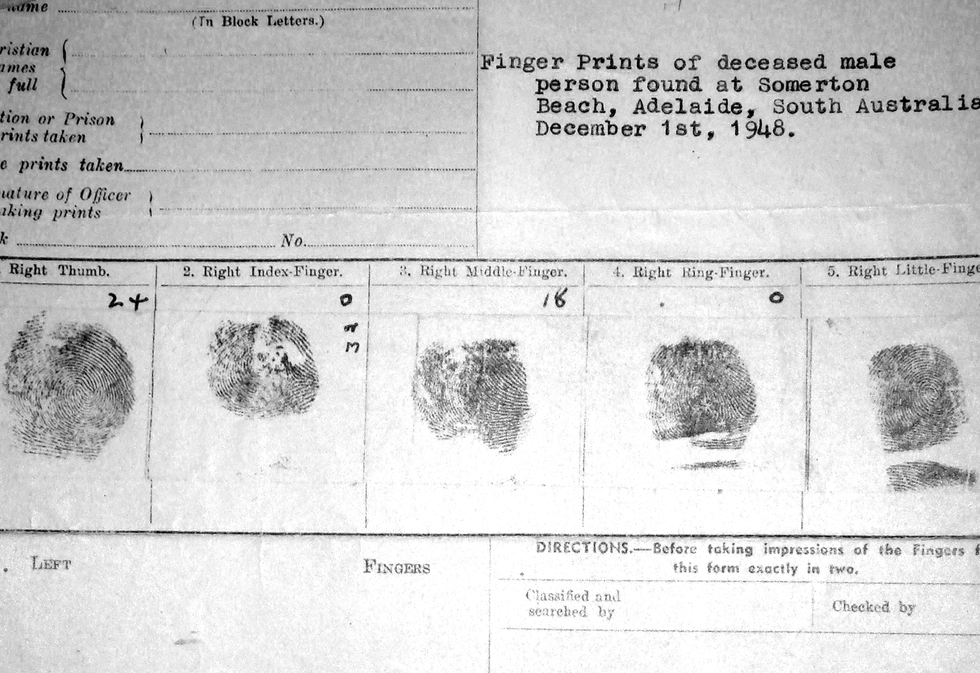 The man’s fingerprints, taken after autopsy, were sent to the U.S. Federal Bureau of Investigation, which found no match.
DEREK ABBOTT
The man’s fingerprints, taken after autopsy, were sent to the U.S. Federal Bureau of Investigation, which found no match.
DEREK ABBOTT
There was speculation of foul play. Perhaps the man was a spy who had come in from the cold; 1948 was the year after the Cold War got its name. This line of thought was strengthened, a few months later, by codelike writings in a book that came to be associated with the case.
These speculations aside, the idea that a person could simply die in plain view and without friends or family was shocking. This was a man with an athletic build, wearing a nice suit, and showing no signs of having suffered violence. The problem nagged many people over the years, and eventually it took hold of me. In the late 2000s, I began working on the Somerton Man mystery, devoting perhaps 10 hours a week to the research over the course of about 15 years.
Throughout my career, I have always been interested in cracking mysteries. My students and I used computational linguistics to identify which of the three authors of The Federalist Papers—Alexander Hamilton, James Madison, and John Jay—was responsible for any given essay. We tried using the same method to confirm authorship of Biblical passages. More recently, we’ve been throwing some natural-language processing techniques into an effort to decode the Voynich Manuscript, an early 15th-century document written in an unknown language and an unknown script. These other projects yield to one or another key method of inquiry. The Somerton Man problem posed a broader challenge.
 News article about the Somerton man case.TROVE PARTNERS
News article about the Somerton man case.TROVE PARTNERS  He was buried by the Salvation Army on 14 June 1949.NEWS CORP./ALAMY
He was buried by the Salvation Army on 14 June 1949.NEWS CORP./ALAMYMy one great advantage has been my access to students and to scientific instruments at the University of Adelaide, where I am a professor of electrical and electronic engineering. In 2009, I established a working group at the university’s Center for Biomedical Engineering.
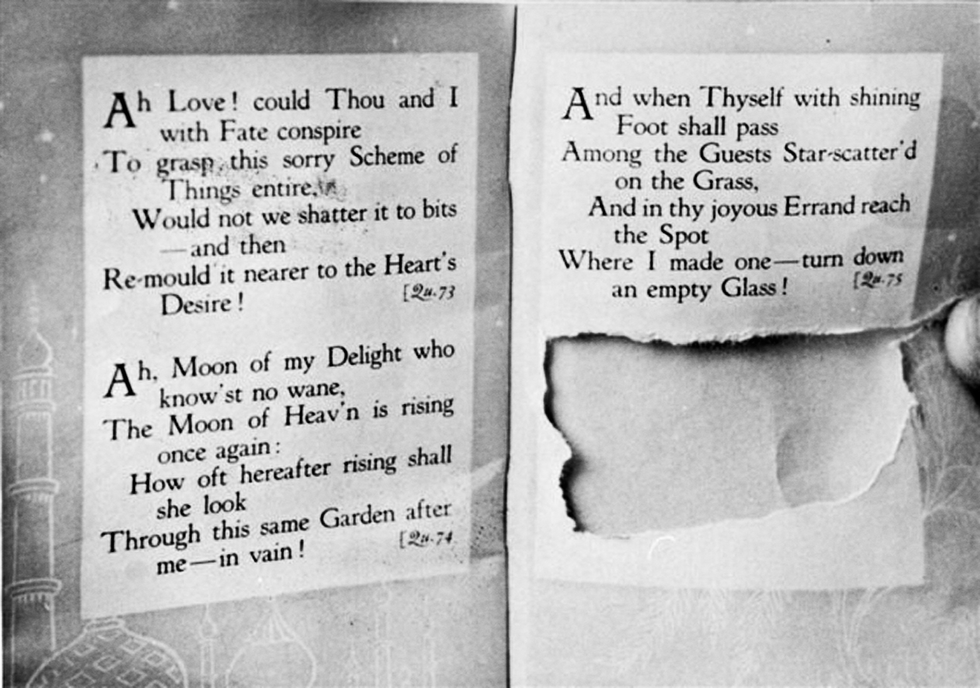
The slip corresponded to the missing part of the final page of the book.
DEREK ABBOTT
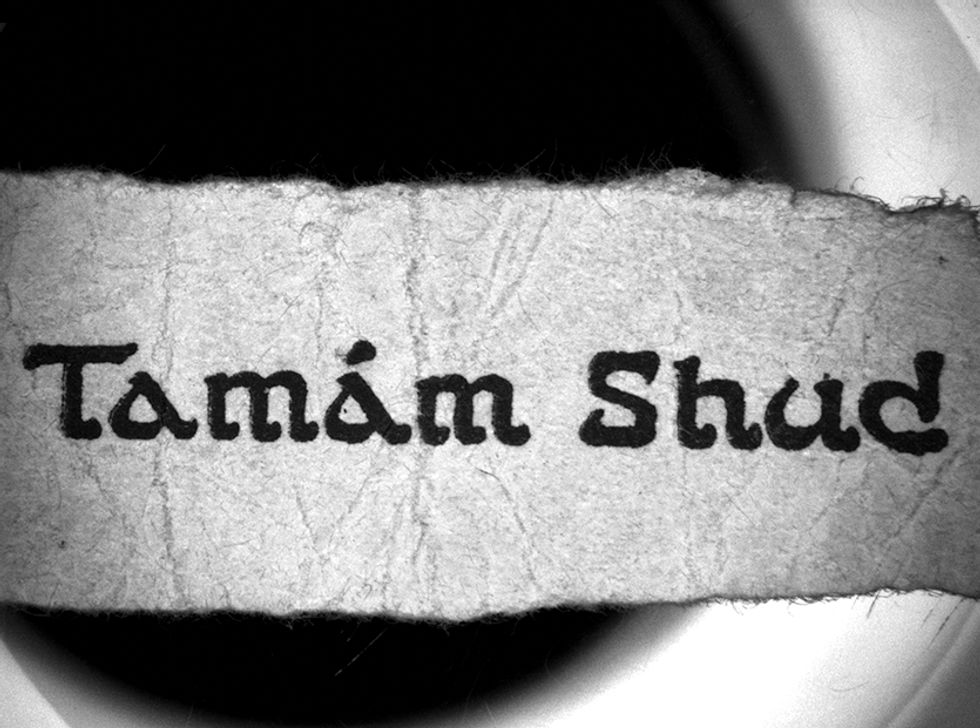
One question surrounding the Somerton Man had already been solved by sleuths of a more literary bent. In 1949, a pathologist had found a bit of paper concealed in one of the dead man’s pockets, and on it were printed the words Tamám Shud, the Persian for “finished.” The phrase appears at the end of Edward FitzGerald’s translation of the Rubáiyát of Omar Khayyám, a poem that remains popular to this day.
The police asked the public for copies of the book in which the final page had been torn out. A man found such a book in his car, where apparently it had been thrown in through an open window. The book proved a match.
The book was linked to the dead man by a slip of paper discovered in his watch pocket; the paper bore two Persian words.
NEWS CORP.
The back cover of the book also included scribbled letters, which were at first thought to constitute an encrypted message. But statistical tests carried out by my team showed that it was more likely a string of the initial letters of words. Through computational techniques, we eliminated all of the cryptographic codes known in the 1940s, leaving as a remaining possibility a one-time pad, in which each letter is based on a secret source text. We ransacked the poem itself and other texts, including the Bible and the Talmud, but we never identified a plausible source text. It could have been a pedestrian aide-mémoire—to list the names of horses in an upcoming race, for example. Moreover, our research indicates that it doesn’t have the structural sophistication of a code. The Persian phrase could have been the man’s farewell to the world: his suicide note.
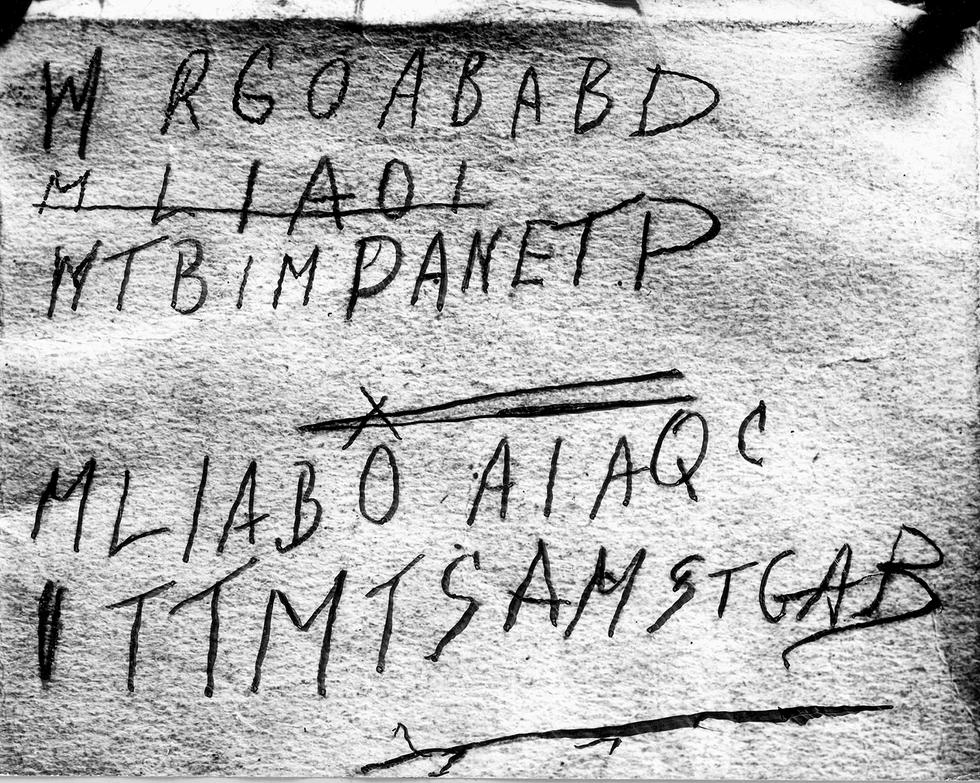
A copy of the Rubáiyát of Omar Khayyám was found months after the death of the Somerton Man. Letters scrawled on the back cover were at first mistaken for code.
WILLIAM R.F. KRISCHOCK
Also scribbled on the back cover was a telephone number that led to one Jo Thomson, a woman who lived merely a five-minute walk from where the Somerton Man had been found. Interviewers then and decades later reported that she had seemed evasive; after her death, some of her relatives and friends said they speculated that she must have known the dead man. I discovered a possible clue: Thomson’s son was missing his lateral incisors, the two teeth that normally flank the central incisors. This condition, found in a very small percentage of the population, is often congenital; oddly, the Somerton Man had it, too. Were they related?
And yet the attempt to link Thomson to the body petered out. Early in the investigation, she told the police that she had given a copy of the Rubáiyát to a lieutenant in the Australian Army whom she had known during the war, and indeed, that man turned out to own a copy. But Thomson hadn’t seen him since 1945, he was very much alive, and the last page of his copy was still intact. A trail to nowhere, one of many that were to follow.

A plaster death mask was molded directly from the cadaver 6 months after death, during which time the facial features had become distorted.
DEREK ABBOTT
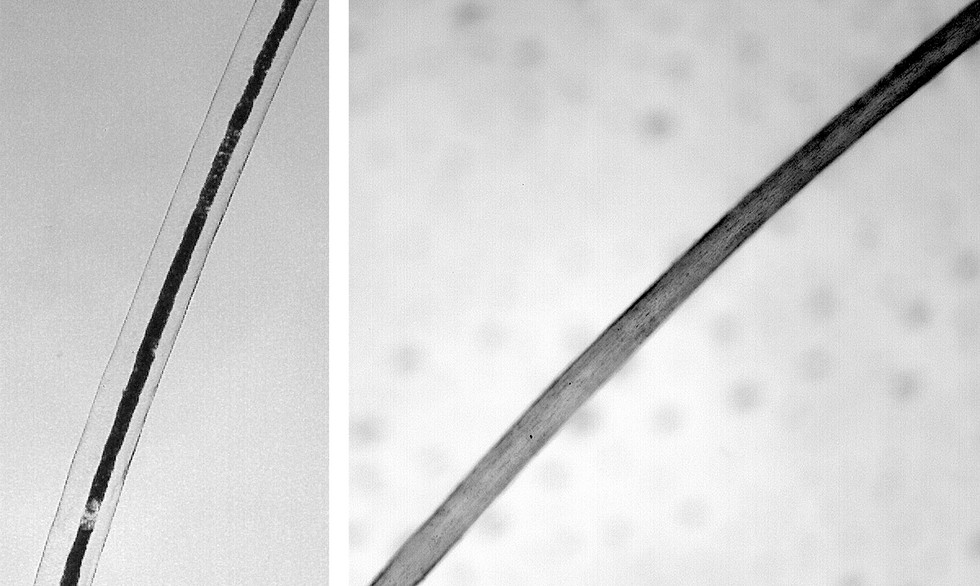
The body was reported to have had graying hair at the sides; this gray hair [left], shown under magnification, was pulled from the mask. A light brown hair was also found [right]; the man had been reported as having “mousey” colored hair.
DEREK ABBOTT
We engineers in the 21st century had several other items to examine. First was a plaster death mask that had been made six months after the man died, during which time the face had flattened. We tried several methods to reconstruct its original appearance: In 2013 we commissioned a picture by Greg O’Leary, a professional portrait artist. Then, in 2020, we approached Daniel Voshart, who designs graphics for Star Trek movies. He used a suite of professional AI tools to create a lifelike reconstruction of the Somerton Man. Later, we obtained another reconstruction by Michael Streed, a U.S. police sketch artist. We published these images, together with many isolated facts about the body, the teeth, and the clothing, in the hope of garnering insights from the public. No luck.
As the death mask had been molded directly off the Somerton Man’s head, neck, and upper body, some of the man’s hair was embedded in the plaster of Paris—a potential DNA gold mine. At the University of Adelaide, I had the assistance of a hair forensics expert, Janette Edson. In 2012, with the permission of the police, Janette used a magnifying glass to find where several hairs came together in a cluster. She was then able to pull out single strands without breaking them or damaging the plaster matrix. She thus secured the soft, spongy hair roots as well as several lengths of hair shaft. The received wisdom of forensic science at the time held that the hair shaft would be useless for DNA analysis without the hair root.

Janette Edson extracted hairs embedded in the plaster death mask.
DEREK ABBOTT

The hairs were then loaded into a laser ablation inductively coupled plasma mass spectrometer, which vaporizes hair along its shaft sequentially.
DEREK ABBOTT
Janette performed our first DNA analysis in 2015 and, from the hair root, was able to place the sample within a maternal genetic lineage, or haplotype, known as “H,” which is widely spread around Europe. (Such maternally inherited DNA comes not from the nucleus of a cell but from the mitochondria.) The test therefore told us little we hadn’t already known. The concentration of DNA was far too low for the technology of the time to piece together the sequencing we needed.
Fortunately, sequencing tools continued to improve. In 2018, Guanchen Li and Jeremy Austin, also at the University of Adelaide, obtained the entire mitochondrial genome from hair-root material and narrowed down the maternal haplotype to H4a1a1a.

This closeup view of the mask shows embedded hairs standing on end.
JANETTE EDSON & DEREK ABBOTT
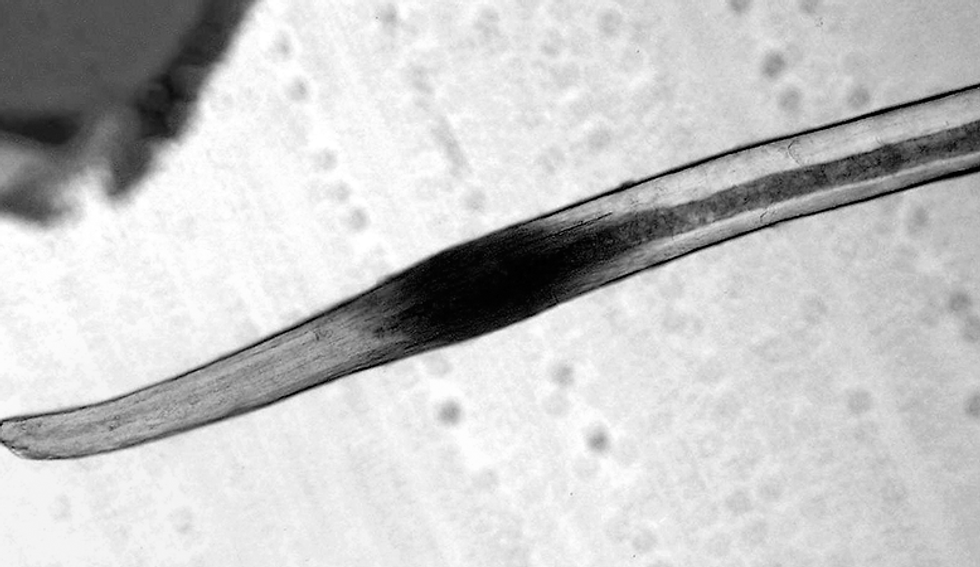
A magnification of the Somerton Man’s hair roots shows a darkened area—a phenomenon known as postmortem banding that can appear a few hours after death.
DEREK ABBOTT
However, to identify Somerton Man using DNA databases, we needed to go to autosomal DNA—the kind that is inherited from both parents. There are more than 20 such databases, 23andMe and Ancestry being the largest. These databases require sequences of from 500,000 to 2,000,000 single nucleotide polymorphisms, or SNPs (pronounced “snips”). The concentration levels of autosomes in the human cell tend to be much lower than those of the mitochondria, and so Li and Austin were able to obtain only 50,000 SNPs, of which 16,000 were usable. This was a breakthrough, but it still wasn’t good enough to work on a database.
In 2022, at the suggestion of Colleen Fitzpatrick, a former NASA employee who had trained as a nuclear physicist but then became a forensic genetics expert, I sent a hair sample to Astrea Forensics, a DNA lab in the United States. This was our best hair-root sample, one that I had nervously guarded for 10 years. The result from Astrea came back—and it was a big flop.
Seemingly out of options, we tried a desperate move. We asked Astrea to analyze a 5-centimeter-long shaft of hair that had no root at all. Bang! The company retrieved 2 million SNPs. The identity of the Somerton Man was now within our reach.
So why did the rootless shaft work in our case?
The DNA analysis that police use for standard crime-solving relies on only 20 to 25 short tandem repeats (STRs) of DNA. That’s fine for police, who mostly do one-to-one matches to determine whether the DNA recovered at a crime scene matches a suspect’s DNA.
But finding distant cousins of the Somerton Man on genealogical databases constitutes a one-to-many search, and for that you typically need around 500,000 markers. For these genealogical searches, SNPs are used because they contain information on ethnicity and ancestry generally. Note that SNPs have around 50 to 150 base pairs of nucleotides, whereas typical STRs tend to be longer, containing 80 to 450 base pairs. The hair shaft contains DNA that is mostly fragmented, so it’s of little use when you’re seeking longer STR segments but it’s a great source of SNPs. So this is why crime forensics traditionally focused on the root and ignored the shaft, although this practice is now changing very slowly.
Another reason the shaft was such a trove of DNA is that keratin, its principal component, is a very tough protein, and it had protected the DNA fragments lodged within it. The 74-year-old soft spongy hair root, on the other hand, had not protected the DNA to the same extent. We set a world record for obtaining a human identification, using forensic genealogy, from the oldest piece of hair shaft. Several police departments in the United States now use hair shafts to retrieve DNA, as I am sure many will start to do in other countries, following our example.
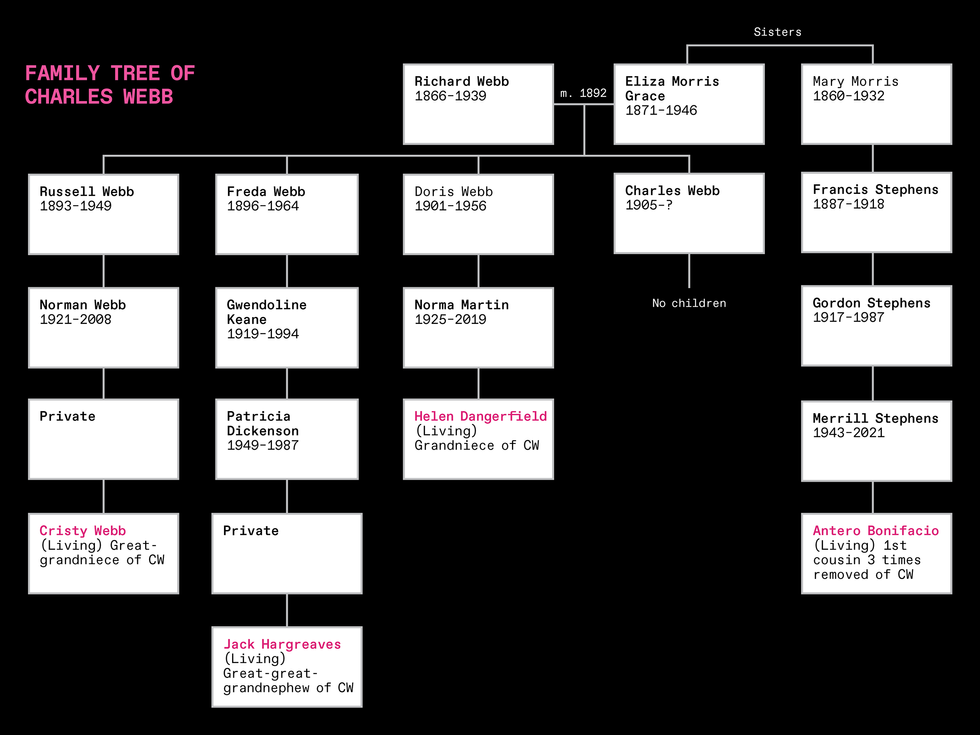 This is the essential part of the family tree that led to the identification of Charles Webb. On the database, the researchers found Jack Hargreaves, who provided the initial DNA match for this segment of the 4,000-person tree. A statistical measure of genetic affinity showed that DNA extracted from the hair was related to that of the four living people shown in pink. Two siblings are not shown, as they did not have descendants.COLLEEN FITZPATRICK & DEREK ABBOTT
This is the essential part of the family tree that led to the identification of Charles Webb. On the database, the researchers found Jack Hargreaves, who provided the initial DNA match for this segment of the 4,000-person tree. A statistical measure of genetic affinity showed that DNA extracted from the hair was related to that of the four living people shown in pink. Two siblings are not shown, as they did not have descendants.COLLEEN FITZPATRICK & DEREK ABBOTTLibraries of SNPs can be used to untangle the branching lines of descent in a family tree. We uploaded our 2 million SNPs to GEDmatch Pro, an online genealogical database located in Lake Worth, Fla. (and recently acquired by Qiagen, a biotech company based in the Netherlands). The closest match was a rather distant relative based in Victoria, Australia. Together with Colleen Fitzpatrick, I built out a family tree containing more than 4,000 people. On that tree we found a Charles Webb, son of a baker, born in 1905 in Melbourne, with no date of death recorded.
Charles never had children of his own, but he had five siblings, and I was able to locate some of their living descendants. Their DNA was a dead match. I also found a descendant of one of his maternal aunts, who agreed to undergo a test. When a positive result came through on 22 July 2022, we had all the evidence we needed. This was our champagne moment.
In late 2021, police in South Australia ordered an exhumation of the Somerton Man’s body for a thorough analysis of its DNA. At the time we prepared this article, they had not yet confirmed our result, but they did announce that they were “cautiously optimistic” about it.
All at once, we were able to fill in a lot of blank spaces. Webb was born on 16 November 1905, in Footscray, a suburb of Melbourne, and educated at a technical college, now Swinburne University of Technology. He later worked as an electrical technician at a factory that made electric hand drills. Our DNA tests confirmed he was not related to Thomson’s son, despite the coincidence of their missing lateral incisors.
 The photograph shows a youthful Charles Webb with his brother Roy and their parents, Dick and Eliza. T. GERALD KEANE
The photograph shows a youthful Charles Webb with his brother Roy and their parents, Dick and Eliza. T. GERALD KEANEWe discovered that Webb had married a woman named Dorothy Robertson in 1941 and had separated from her in 1947. She filed for divorce on grounds of desertion, and the divorce lawyers visited his former place of work, confirming that he had quit around 1947 or 1948. But they could not determine what happened to him after that. The divorce finally came through in 1952; in those days, divorces in Australia were granted only five years after separation.
At the time of Webb’s death his family had become quite fragmented. His parents were dead, a brother and a nephew had died in the war, and his eldest brother was ill. One of his sisters died in 1955 and left him money in her will, mistakenly thinking he was still alive and living in another state. The lawyers administering the will were unable to locate Charles.

These two mass spectrographs compare hairs from the Somerton Man [blue] and from contemporary reference hair material [red]. The spectrograph for arsenic [left] shows an insignificantly elevated level in the Somerton Man. Note that the Somerton Man’s hair sample is 1 centimeter long, which represents about a month’s growth. The spectrograph for lead [right] dropped from a high level in the month before death, a clue that his routine changed during that time.
JAMES CHAPPELL & DEREK ABBOTT
We got more than DNA from the hair: We also vaporized a strand of hair by scanning a laser along its length, a technique known as laser ablation. By performing mass spectrometry on the vapor, we were able to track Webb’s varying exposure to lead. A month before Webb’s death, his lead level was high, perhaps because he had been working with the metal, maybe soldering with it. Over the next month’s worth of hair growth, the lead concentration declined; it reached its lowest level at his death. This might be a sign that he had moved.
With a trove of photographs from family albums and other sources, we were able to compare the face of the young Webb with the artists’ reconstructions we had commissioned in 2013 and 2021 and the AI reconstruction we had commissioned in 2020. Interestingly, the AI reconstruction had best captured his likeness.

Daniel Voshart used AI-based software to produce this reconstruction of Charles Webb’s appearance.
DANIEL VOSHART
A group photograph, taken in 1921, of the Swinburne College football team, included a young Webb. Clues found in newspapers show that he continued to participate in various sports, which would explain the athletic condition of his body.
What’s interesting about solving such a case is how it relies on concepts that may seem counterintuitive to forensic biologists but are quite straightforward to an electronics engineer. For example, when dealing with a standard crime scene that uses only two dozen STR markers, one observes very strict protocols to ensure the integrity of the full set of STRs. When dealing with a case with 2 million SNPs, by contrast, things are more relaxed. Many of the old-school STR protocols don’t apply when you have access to a lot of information. Many SNPs can drop out, some can even be “noise,” the signal may not be clean—and yet you can still crack the case!
Engineers understand this concept well. It’s what we call graceful degradation—when, say, a few flipped bits on a digital video signal are hardly noticed. The same is true for a large SNP file.
And so, when Astrea retrieved the 2 million SNPs, the company didn’t rely on the traditional framework for DNA-sequencing reads. It used a completely different mathematical framework, called imputation. The concept of imputation is not yet fully appreciated by forensics experts who have a biological background. However, for an electronics engineer, the concept is similar to error correction: We infer and “impute” bits of information that have dropped out of a received digital signal. Such an approach is not possible with a few STRs, but when handling over a million SNPs, it’s a different ball game.
Much of the work on identifying Charles Webb from his genealogy had to be done manually because there are simply no automated tools for the task. As an electronics engineer, I now see possible ways to make tools that would speed up the process. One such tool my team has been working on, together with Colleen Fitzpatrick, is software that can input an entire family tree and represent all of the birth locations as colored dots on Google Earth. This helps to visualize geolocation when dealing with a large and complex family.
The Somerton Man case still has its mysteries. We cannot yet determine where Webb lived in his final weeks or what he was doing. Although the literary clue he left in his pocket was probably an elliptical suicide note, we cannot confirm the exact cause of death. There is still room for research; there is much we do not know.
This article appears in the April 2023 print issue as “Finding Somerton Man.”

These SEM images of a microscopic octahedral truss structure are shown at 100-micrometer scale [left] and zoomed in at 10-µm scale [right], where the yellow structure shows an individual unit cell.
However, two-photon lithography has proven too slow and expensive for large-scale practical applications. This has largely rendered it an expensive laboratory tool to produce microscopic prototypes.
The new method can manufacture complex, microscopic 3D objects such as letters, numbers, rings, lenses, and gears that can be remotely controlled by applying a magnetic field.
Previous research has sought to split the laser beam used in two-photon lithography into multiple focal points to speed up fabrication. However, this strategy typically still achieves printing speeds of only about 10,000 voxels per second and less than 0.1 cubic millimeters per hour. Moreover, this approach is usually not able to control each individual laser’s focus, and so cannot produce highly variable structures.
Now a new two-photon lithography technique can print nanoscale 3D objects at speeds of up to 2 million voxels per second and 4.5 to 54 cubic millimeters per hour. In addition, it achieved a resolution of up to 90 nanometers, the best seen yet in high-throughput two-photon lithography, the scientists noted. Moreover, the team’s new process can simultaneously operate up to 2,000 individually programmable laser foci to fabricate complex structures, the most seen yet in high-throughput two-photon lithography, they added.
“The increase in throughput means the cost is substantially reduced, and the technology can now be used for industrial-scale applications at a more reasonable price and fabrication rate,” says study senior author Shih-Chi Chen, an optical scientist and mechanical engineer at the Chinese University of Hong Kong.
Solidifying the resin used in two-photon lithography requires extremely high laser intensities. Using multiple laser foci increases the laser power required, and the lasers typically used in two-photon lithography can barely provide the power needed to support more than 50 foci. In contrast, the new method used a near-infrared laser with a peak power of approximately 10 gigawatts.
Usually, two-photon lithography relies on foci that receive about 10,000 low-power laser pulses in order to fully solidify a voxel. However, the new technique uses a laser that fires tens to hundreds of thousands of times slower than the lasers typically used in two-photon lithography. To compensate, the new technique uses a single pulse to solidify each voxel. This required significant tinkering with the light-sensitive resin to optimize its printing quality, the scientists said.
“We achieved the best resolution with single-pulse exposure, which is totally opposite to the conventional approach to achieve high resolution—that is, low average power and long exposure time,” Chen says.
The new method fires a thousand 100-femtosecond-long pulses per second, bouncing these pulses off a digital micromirror device that displays a hologram. The scientists could use the hologram to divide each laser pulse into up to 2,000 foci with individually controllable strength, location and phase that could operate simultaneously in parallel.
In experiments, the researchers showed their new method could manufacture complex, microscopic 3D objects such as letters, numbers, rings, lenses, and eggbeater-like structures. They also fabricated magnetic gears they could remotely control by applying a magnetic field.
 These 14 images reveal the range of nanostructures the new holographic technique can fabricate, including magnetic nanoscale gear wheels that could be remotely moved by applying a magnetic field [insets m and n].Chinese University of Hong Kong
These 14 images reveal the range of nanostructures the new holographic technique can fabricate, including magnetic nanoscale gear wheels that could be remotely moved by applying a magnetic field [insets m and n].Chinese University of Hong Kong
In the new study, the scientists also revealed they could modify the laser power of each focus to achieve 11 different intensity levels. This “gray-scale control” may find use in adjusting the solidity and mechanical properties of each voxel. The new technique displayed gray-scale control with an accuracy of more than 99 percent, the highest seen yet in parallel two-photon lithography, the scientists noted.
In addition, the researchers reported, the new method yields the highest energy efficiency yet in two-photon lithography. Whereas other techniques demand an operating power of roughly 1.5 to 4 watts, the new method requires only an average power of 400 milliwatts to operate 2,000 foci.
One potential application for nanoscale 3D printing is fabricating metastructures—materials whose structures possess repeating patterns at scales that are smaller than the wavelengths of whatever force they are designed to influence. Optical metastructures, which are designed to manipulate electromagnetic radiation, can bend light in unexpected ways, resulting in invisibility cloaks and other devices.
One of the greatest challenges with research into metastructures is manufacturing objects containing subfeatures less than a micrometer in size but, on the whole, are many thousands of times as large as their subfeatures. In experiments, the scientists revealed their new technique could fabricate a grid roughly 1 cubic millimeter in size made up of more than 680,000 cells with subfeatures as small as 700 nanometers.
The researchers are now exploring using AI to generate optimal fabrication procedures with their new technique. The aim is for the products to “have better structural integrity, strength, and uniformity,” Chen says.
The scientists detailed their findings online 27 March in the journal Nature Communications.

Thornhill Medical's mobile life-support device, called MOVES SLC, has been used by military medical teams for five years. The unit can be slung across the shoulder and includes a circle-circuit ventilator and oxygen concentrator that eliminate the need to carry heavy, dangerous high pressure O2 cylinders.
Meanwhile, the studies conducted by Dr. Fisher started drawing attention from the U.S. Marines. They had been looking for solutions to reduce the use of large, heavy, and potentially explosive oxygen tanks transported by their medical teams to military operation sites.
“At first, they asked us if we could prove that it was possible to ventilate patients using much less oxygen,” says Veso Tijanic, COO of Thornhill Medical. “We proved it. Then, they asked us whether we could develop a device for this. Finally, whether we could integrate other functionalities into this device.”
The device is currently saving lives in Ukraine, Thornhill Medical having donated a number of them as well as its mobile anesthesia delivery module MADM.
These back-and-forths lasted about five years, gradually combining science and technology. It resulted in a very first product, launched in 2011: MOVES, an innovative portable life support unit.
This cooperation has also deeply transformed Thornhill Medical.
“We used to see ourselves as an R&D laboratory, we have now also become a medical device manufacturer!” says Tijanic.
Whilst the U.S. Marines started using MOVES, Thornhill Medical continued to innovate. In 2017, it launched an enhanced version, MOVES SLC.
Today, the Canadian company employs a staff of about 70. It continues to do research and development with its own team and partners around the world, publishing regularly in scientific journals. It has sold MOVES SLC around the world and launched two other solutions, MADM and ClearMate.
MADM is a portable device (capable of functioning on extreme terrain) which connects to any ventilator to deliver gas anaesthesia. ClearMate is an instrument — also portable and without electricity — which allows to take quick action in case of carbon monoxide poisoning. This is the most common respiratory poisoning, where every second without treatment worsens consequences on the brain and other organs.
Just like these two products, the heart of MOVES SLC is a technology stemming directly from Dr. Fisher’s research in breathing sciences. It includes a ventilator operating in circle-circuit: It recovers the oxygen expired by the patient, carefully controls its concentration (high FiO2) and redistributes only the strict minimum to the patient.
MOVES SLC operates with significantly less oxygen than required by traditional open-circuit ventilators. This is so little that a small oxygen-concentrator — integrated into MOVES SLC, that extracts oxygen from ambient air — is sufficient. No need for supplies from large oxygen tanks.
Yet, MOVES SLC is more than an innovative ultra-efficient ventilator, says Tijanic: “It is a complete life support device.” In addition to its integrated oxygen concentrator, it also includes suction and several sensors that monitor vital signs and brings it all together via a unique interface that can be operated on the device or by a mobile touch screen.

The MOVES SLC unit includes a ventilator operating in circle-circuit: It recovers the oxygen expired by the patient, carefully controls its concentration and redistributes only the strict minimum to the patient. The device also includes a small oxygen concentrator, suction, and several sensors that monitor vital signs.
Thornhill Medical
The user can intubate a patient and monitor its ventilation (FiO2, ETCO2, SpO2, ABP and other indicators) in addition to the patient’s temperature (two sensors), blood pressure (internal and external) and 12-lead ECG. The evolution of these measurements can be followed over the last 24 hours.
All of this, in a device measuring only 84 cm x 14 cm x 25 cm, weighing about 21 kilograms (including interchangeable batteries) which can be slung across the shoulder.
“MOVES must function in the middle of military operations, and be resistant to vibrations, crashes and shock, continue operating smoothly in sandstorms or in the rain.”
—Veso Tijanic, COO of Thornhill Medical
“MOVES SLC represents no more than 30 percent of the volume and weight of traditional equipment — ventilator, concentrator, suction, monitoring device,” adds the COO. Integrating various technologies in such a lightweight, compact package was, without surprise, a major challenge for the engineers. Still, not the most difficult one.
Making medical device components capable of withstanding extreme conditions will have been even more complex. “Traditional technologies were designed to function in hospitals,” explains Tijanic. “MOVES must function in the middle of military operations, and be resistant to vibrations, crashes and shock, continue operating smoothly in sandstorms or in the rain, in temperatures between -26°C and +54°C.”
Sometimes, the engineers could take existing components and develop protective features for them. Occasionally, they would recast them from different markets (oxygen sensors, for instance) to integrate them into their device. And in other cases, they had to start from scratch, creating their own robust components.
The challenge was successfully overcome: “MOVES is designed under the highest industry standards and has been tested and fully certified by various regulatory bodies.” It has been certified MIL-STD-810G, a ruggedness U.S. military standard, verified by over twenty different tests (acoustic vibration, explosive atmosphere, etc.).
The device is hence approved for use — not only transported, but actually used on a patient — in various helicopters, aircraft and land vehicles. And this makes a world of difference for Tijanic. “Critical care, such as we provide, normally requires specially equipped facilities or vehicles. With MOVES SLC, any place or vehicle — even civilian — of sufficient size, is an opportunity for treatment.”
Thornhill’s fully integrated mobile life support has been used by military medical teams for five years already. The device is currently saving lives in Ukraine, Thornhill Medical having donated a number of them as well as its mobile anesthesia delivery module MADM.
In July 2022, the U.S. Army published a report summarizing its medical modernization strategy. The 22-page report confirms the need for ever more lightweight, compact, and cost-effective technology. It also mentions the use of artificial intelligence for more autonomous monitoring of the patients’ medical condition. Thornhill is exploring the AI angle.
“There isn’t always a qualified expert available everywhere,” explains Tijanic. “AI could ensure the optimum settings of the device, and then modify these depending on how the patient’s condition evolves.”
Thornhill is also exploring another solution for cases where no experts are available on spot. Last April, a MOVES SLC was used in a demonstration of “remote control of ventilators and infusion pumps to support disaster care.” Operators based in Seattle successfully controlled remotely a device based in Toronto. Science-fiction thus becomes science, and turns into reality.
The Canadian company continues innovating to heal and save lives on rough chaotic terrain and in the most extreme and unpredictable circumstances. It is driven by medical and technological progress. It is also driven by a many-thousand-year-old trend: Humans will likely never stop waging war.








